Recommendations for Ensuring Equitable Access and Quality
To the New York State Departments of Health and Insurance:
The Opportunity Agenda would like to thank Governor Eliot Spitzer, Commissioner of Health Richard Daines, and Superintendent of Insurance Eric Dinallo for the chance to contribute to the development of a comprehensive and equitable health care system in New York. Please find included written testimony and recommendations, submitted on behalf of The Opportunity Agenda, for your New York City public hearing today, “Increasing Access to Health Insurance Coverage and Moving Toward Universal Healthcare Coverage.”
If you have any questions or would like further information, please use the following contact information:
Kevin Shawn Hsu
Associate Counsel
568 Broadway, Suite 302
New York, NY 10012
212.334.4267
[email protected]
Thank you for your consideration of this testimony.
Sincerely,
Kevin Hsu
Associate Counsel
Recommendations for Ensuring Equitable Access and Quality in New York State Health Care System Reform
Submitted to the New York State Departments of Health and Insurance by The Opportunity Agenda
October 30, 2007
The Opportunity Agenda welcomes the chance to provide testimony to the Departments of Health and Insurance to assist in the development of a health care system that provides equal access to high-quality care for all New Yorkers.
This testimony seeks to provide New York with equity benchmarks, elements of state-level health care policies and proposals that promote equitable health care access and quality for all populations, that should be used in evaluating any health care system reform proposals. The benchmarks address six aspects of the health care system: (1) Access to Health Care, (2) Quality of Care, (3) Patient Empowerment, (4) Health Care Infrastructure, (5) Policy Infrastructure, (6) Social and Community Determinants of Health. These benchmarks are informed by our review of literature on health care disparities and draw from existing and proposed state-level policies that promote equitable, high-quality health care for all.
Summary of Recommendations
In crafting a universal health care system that provides access to quality care for all residents of New York, the State should include reforms that ensure improvements to the system for all while eliminating health care disparities based on race, ethnicity, primary language and income. New York should utilize the equity benchmarks described in this testimony to evaluate any health care system reform proposal. In making health care affordable and accessible to all, including underserved communities, a health care system must ensure that cost-sharing policies are equitable by, for example, preventing policies such as premium pricing based on existing health status or individual mandates from disproportionately excluding communities of color from care. Reforms must also improve the cultural and linguistic competency of both providers and health care systems to encourage effective use of health care resources and delivery of appropriate care. In all of these efforts, New York must also integrate monitoring efforts into reforms to guarantee that changes lessen, rather than exacerbate health care disparities.
New York must also improve the quality of care that patient receive, regardless of the insurance program in which they are enrolled. With regards to eliminating the documented inequities in the quality of health care received by communities of color, immigrant communities, and low- income populations in New York, reforms must include collection of quality of care data, stratified by race, ethnicity, primary language and other characteristics of underserved communities. This data should be publicly reported and, more importantly, acted upon by providing incentives to providers who engage in quality improvement programs targeting demonstrated health care disparities, educating patients, and supporting and expanding community health worker programs that bridge cultural and trust gaps between providers and underserved communities.
Finally, New York must reform the health care system infrastructure to better address the needs of racial, ethnic, and language minorities. This includes increasing state support for and reducing the financial vulnerability of “safety net” hospitals, community health centers, and health care institutions serving poor and minority communities. Reforms should also construct or revive programs that combat disparities, such as creating incentives for health care professionals working in underserved communities, reviving the statewide network of Health Systems Agencies that used community health planning to better align community needs and health care resources, and reviewing the use of the Certificate of Need process so that changes to hospital services are contingent on community need and reduction of racial, ethnic, and linguistic health disparities. To implement these infrastructure and policy reforms, New York should dedicate resources to coordinating the various responsible state agencies in creating a comprehensive, statewide approach to eliminating racial and ethnic health disparities.
Legal and Ethical Principles
Our review of New York’s constitutional, statutory and other legal obligations, as well as public opinion, indicate that efforts to reform New York’s health care system must be informed by the following principles:
- That the New York State Constitution obligates the State to provide access to high quality health care to all New York residents, with particular attention to vulnerable groups and those least able to pay for care.1
- That federal civil rights laws and international human rights laws obligate the State, its subdivisions, and virtually all health care providers to avoid and actively dismantle any practices having a discriminatory purport or effect on particular racial, ethnic, or linguistic groups, with respect to access to or quality of health care.2
- That federal and state health care laws obligate the State to ensure adequate support and care for low-income and medically underserved communities, including through adequate Medicaid reimbursement rates and equal treatment, irrespective of income or insurance status.3
- That the people of New York overwhelmingly believe that everyone in New York has a right to health care, and that the State is responsible for ensuring that racial or ethnic minorities and low-income New Yorkers have an equal chance to access health care as do wealthy people.4
- That protecting and promoting the health of the inhabitants of New York5 requires systems, policies, and practices that ensure equitable access to high quality care.6
Health Care Equity in New York
The efforts of Governor Eliot Spitzer, the Department of Health, and the Department of Insurance to move New York toward universal health coverage are to be lauded. Rapidly escalating health care costs, a rising number of people who lack health insurance, inconsistent health care quality, and a paucity of federal action to address these problems necessitates the consideration of state-level health care reform proposals that, if enacted, would create significant changes in how the State approaches health insurance coverage and health system regulation.7 A poll conducted by The Opportunity Agenda and designed by researchers at the Harvard School of Public Health confirms public support for these efforts: 89% surveyed said that “everyone in New York has a right to health care.”8
The New York State Departments of Health and Insurance are holding these hearings with the explicit goals of achieving universal, high-quality health insurance coverage and containing health care costs. However, a major problem which impacts both cost and quality, yet is often unaddressed, is the problem of inequality in health care access and quality. Inequality is a pervasive and persistent problem that is acknowledged by health care quality and policy experts to be a central concern in any heath care reform effort.9 We use the term health care inequality to describe disparate or disproportionate health care access and quality problems experienced by racial and ethnic minorities, the uninsured, immigrants, those who are not proficient in English, and others, relative to more advantaged groups. While having health insurance is the single most significant factor determining the timeliness and quality of health care that patients receive, inequality persists even among similarly insured patients. For example, a large body of research demonstrates that even with the same health problems and the same sources of health insurance, racial and ethnic minority patients, as well as those who are not proficient in English, tend to receive a lower quality of health care.10
Health care disparities are intimately linked to access, quality, and cost issues within the health care system. For example, a relatively small investment targeted toward communities experiencing significant gaps in care can save the State significant amounts of money. Consider the neighborhood of Rockaway, Queens, where 13.5% of mothers receive late or no prenatal care; unsurprisingly, a full 10% of babies in that community are born low-weight.11 While the average cost of medical and follow-up care for a healthy normal weight baby is $6,500, care for a premature or low birth-weight baby costs between $90,000 and $180,000. However, a $180,000 health promotion program will provide more than 50 at-risk pregnant women with intervention to reduce their risk of bearing low birth-weight babies; if the program is even modestly successful, it would dramatically improve the financial efficiency, as well as the quality, of the neighborhood’s health care system.12 New York State could save hundreds of millions of dollars if it ensured access to quality primary care for all New Yorkers.13 True high- quality, universal care requires recognition and efforts to eliminate the significant health care inequities facing residents of New York.
Racial and ethnic minority and language-minority groups face well-documented problems in both accessing health care and receiving equal quality care. Lack of health insurance is a primary cause of these disparities; over half of the nation’s 47 million uninsured individuals are people of color.14 In New York City, 30% of New Yorkers of color are uninsured, compared to under 17% of white New Yorkers.15 And in New York State, Asian residents are more than twice as likely to be uninsured, and Hispanic residents are more than three times likely to be uninsured as non-Hispanic Whites (Figure 1).
Figure 1: Uninsured Rate in New York State, Adults 18-64 By Race, 2007
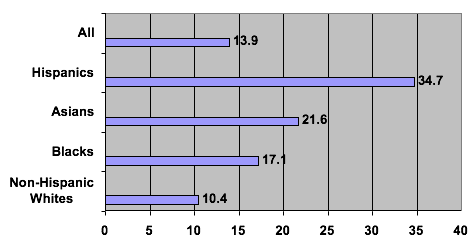
Source: New York State Department of Health, New York State Minority Health Surveillance Report, Sept. 2007; “All races” comes from the Current Population Survey Annual Social and Economic Supplement, available from the Current Population Survey Table Creator at http://www.census.gov/hhes/www/hlthins/data_access.html.
Closing racial and ethnic gaps in insurance coverage while increasing overall insurance rates is crucial. But health insurance coverage expansions alone do not ensure that medically- underserved, predominantly-minority communities will receive quality care in a timely fashion, or that inequality in health care access and quality will be eliminated. Predominantly minority communities also face higher rates of health problems, but have fewer health care resources, such as hospitals, primary care providers, outpatient clinics, and nursing home facilities.16 The health care services that are available to them are often of lower quality than those in more advantaged communities.17 And even among minorities who have insurance, many face cultural and/or linguistic barriers to accessing care, despite the existence of federal standards for cultural and linguistic competence in health care settings.18
As described below, in addition to providing truly universal health insurance coverage, steps toward ending inequality can include collecting data and monitoring for inequality, improving the health care infrastructure in low-income communities and communities of color, and addressing these groups’ cultural and linguistic needs.
I. Access to Health Care
New York can expand access for underserved populations by:
Making health care affordable
Seeing that health care is affordable for all communities necessitates that policies take into account and attempt to minimize the disproportionate impact that health care costs may have on access and utilization among underserved populations. In creating a cost-effective and sustainable economic model for a health care system, New York should be sensitive to the potential effect of proposals on health insurance coverage and access among communities of color. Specifically, New York should:
- Examine the equity of health insurance premium pricing. For example, charging people in poor health more for insurance than those in good health is inequitable, and disproportionately burdens communities of color.
- Consider the equity of cost-sharing arrangements. Cost-sharing arrangements are intended to make costs more transparent and promote cost-conscious consumer behavior, but may thwart universal coverage and exacerbate disparities. Several studies demonstrate that minority and low-income communities are less likely to access health care as out-of-pocket costs rise.19
- Enable those with low incomes to purchase health insurance through sliding fee scales for premiums, public subsidies, and limits on co-payments and other out-of-pocket costs such that those at the lowest income levels will face only nominal charges.
- After implementing any cost-sharing policies, study and respond to potential unintended effects of cost-sharing on utilization by currently uninsured and underinsured groups.
Assessing the differential impact of individual mandates on communities of color, immigrants, and low-income populations
Massachusetts’ new statute to achieve universal coverage requires individuals and families to purchase health insurance, and also establishes standards of affordability to determine premium or cost-sharing contributions. The impact of a similar individual mandate and definitions of affordability here in New York may vary across racial and ethnic groups, even at the same income level, as these groups vary in wealth and access to resources.20 In addition, the challenges of enforcing an individual insurance mandate across different communities are significant. Some documented immigrants, for example, may be reluctant to apply for public health insurance programs, even if eligible, as a result of anti-immigrant rhetoric and policies, and might therefore be slower to comply with a mandate.21 If New York chooses to apply an individual mandate, it should monitor insurance take-up among previously uninsured people by race, ethnicity and immigration status, and take steps to correct policies that might have a disproportionate impact.
Promoting cultural and linguistic competence in health care settings
Health care providers and systems must be culturally and linguistically competent to improve health care access and quality for an increasingly diverse U.S. population.22 The federal Culturally and Linguistically Appropriate Services (CLAS) standards identify fourteen benchmarks that have been widely accepted and increasingly adopted by health systems and providers.23 Indeed, federally-funded health care organizations are mandated to meet four of the standards.24 Similarly, greater diversity among health care professionals is associated with greater access to and satisfaction with care among patients of color.25 New York must develop or expand diversity efforts, which improve the cultural competence of health systems and increase the likelihood that patients of color will access and be satisfied with the health care they receive. Specifically, New York may:
- Promote cultural and linguistic competence through policies that encourage and reward health care organizations that implement the CLAS standards, such as fully reimbursing providers for language services through the Medicaid and Child Health Plus programs, or increasing payments through these programs for providers complying with the full set of standards.
- Promote greater diversity among health care professionals by developing or expanding tuition-for-service agreements with underrepresented health care professionals.
Requiring cultural competency training for health care professional licensure
New York State is one of the most diverse states in the country, and New York City’s population is predominantly people of color. Demographic changes require that the health professions keep pace by training future and current providers to manage diversity in their practice.26 Some states have taken action to address this need—as of 2005, New Jersey required that all physicians practicing in the state must attain minimal cultural competency training as a condition of licensure. New York should assess whether and how various health care expansion proposals should follow suit.
Reducing “fragmentation” of the health insurance market
A potentially significant source of racial and ethnic health care disparities among privately insured populations lies in the fact that minorities who have insurance are likely to be disproportionately enrolled in “lower-tier” health insurance plans. Such plans tend to limit services, offer fewer covered benefits, and have relatively small provider networks. These limitations can impair access to quality care.27 New York can take steps as part of coverage expansion proposals to improve access to the same health care products and services, regardless of coverage source. For example, one proposed California plan, AB 8, provides for the Insurance Commissioner to approve no more than five standardized plans for both public and private insurance markets, allowing patients to make fully-educated decisions about both the cost and quality of benefits each plan will provide.28
Improving and streamlining enrollment procedures for public health insurance programs
Racial and ethnic minorities and immigrants are underrepresented, relative to eligibility rates, in public health insurance programs. States that have achieved greater success in increasing minority participation in public programs have developed and sustained aggressive outreach programs and have taken steps to improve and streamline enrollment, with particular attention to the needs of cultural and language-minority groups.29 New York can improve and streamline enrollment through policies that evaluate and improve enrollment procedures among eligible yet underserved groups. For example, New York can utilize media campaigns, community-based outreach and application assistance, identification of potential enrollees through other systems (such as school lunch, early childhood education, etc.), and simplified enrollment systems.
Consistently evaluating outreach to and enrollment of underserved groups in public health insurance programs
Measurement of public insurance take-up rates in low-income communities and communities of color is an important step to ensure that health care expansion efforts reach underserved groups. By regularly conducting such evaluations and responding to gaps and shortfalls, New York can expect to see improved coverage rates among eligible populations.30
II. Quality of Care
New York seeks to expand health care quality, as well as access. The State can provide incentives for quality improvement, such as pay-for-performance programs, performance measurement, and report cards. But quality improvement efforts that fail to take into account the different challenges and needs of underserved communities, and the health care institutions that serve them, can unintentionally worsen health care quality gaps. To prevent unintentional exacerbation of inequities, New York should establish mechanisms for promoting equity and accountability by promoting the collection of data on health care access and quality by patients’ race, ethnicity, income or education level, and primary language, and by publicly reporting this information.
New York can establish mechanisms for ensuring quality care and accountability to all communities by:
Requiring public and private health systems to collect data revealing and monitoring racial/ethnic, language status, and income-based health care disparities
Currently, state data collection efforts with regard to health care disparities are uneven. New York requires recipients of state funding (e.g., Medicaid managed care organizations) to collect and report health care access and quality data by patient demographic factors, but fails to utilize its leverage as a regulator, payer, and plan purchaser to require all health systems to collect and report data using consistent standards.31 And given that New York has non-discrimination laws that apply to health care settings and require state diligence to enforce, requirements to collect and report standardized data are an important benchmark for efforts to reduce health care inequality. New York should ensure that state health care expansion proposals mandate participation by all health systems operating in the state in a standardized data collection program.
Publicly reporting health care access and quality disparities
Once New York has obtained health care access and quality data by patient demographic characteristics, this information should be publicly reported, to promote greater public accountability, to allow consumers to make more informed decisions about where to seek care, and to assist state efforts to appropriate action to investigate potential violations of law.32
Encouraging the adoption of quality improvement programs that consider the health care challenges and needs of underserved communities
State health care quality improvement efforts, such as pay-for-performance or performance measurement, are gaining increasing attention. But because underserved communities typically face greater health needs and barriers to treatment, performance measurement that is blind to the additional challenges in providing health care to these communities can inadvertently dampen provider enthusiasm for treating low-income communities or communities of color. Quality improvement efforts should take into account the challenges and needs of underserved communities and reward efforts that reduce disparities and improve patient outcomes relative to baseline measures.33 New York should ensure that health care expansion proposals emphasize disparities reduction efforts and avoid unfairly penalizing providers in underserved communities while holding them and health systems accountable for improvements in health outcomes.
III. Patient Empowerment
Patients should be empowered to make decisions about their health care and to insist that care be delivered in a manner consistent with their health care needs, economic status, and cultural context. These issues are particularly relevant for racial and ethnic minority and immigrant patients, who may face significant cultural barriers in U.S. health care settings.34 These concerns can be addressed by:
Developing and strengthening patient education programs that are well-researched and are tailored to the need of underserved communities
Patient education programs commonly seek to help patients understand how to best access health care services and participate fully in treatment plans. Such efforts to empower patients can help reduce health care disparities by providing patients with skills to effectively navigate health care systems and ensure that their needs and preferences are met. For example, patient education programs have been found to be effective as a means of reducing racial and ethnic disparities in pain control.35 Patient education programs are most effective when designed in partnership with community members and groups and when language, culture, and other concerns faced by communities of color are fully addressed.36
Supporting and expanding community health worker programs
Community health workers, also known as lay health navigators or promotoras, are trained members of medically underserved communities who work to improve community health outcomes. Community health worker programs train individuals to teach disease prevention, conduct simple assessments of health problems, and help their neighbors access appropriate health and human resources.37 New York State currently has 23 community health work programs, focused on prenatal and early childhood health.38 Research and practice indicate that such services can improve patients’ ability to access care and understand how to manage illness. Most importantly, community health workers can help reduce health disparities by community mistrust of health care providers stemming from historical discrimination, breaking down cultural divides between providers and patients, assisting in obtaining health insurance and accessing care, and disseminating vital health information to underserved communities.39 From a health care system perspective, community health workers also improve quality and reduce costs by encouraging more appropriate use of health care resources and reducing uncompensated care.40 New York can build on the successes of its existing perinatal community health worker programs by providing grants, seed funding, or other resources to help stimulate community health worker programs in new areas of health disparities, such as diabetes, HIV/AIDS, and preventable ambulatory care sensitive conditions such as asthma, hypertension, and pneumonia.
IV. State Health Care Infrastructure
The disproportionate lack of health insurance among racial and ethnic minorities is associated with lower levels of health care resources (e.g., practitioners, hospitals and health care centers) in communities of color. Even if New York achieves universal health insurance coverage, communities of color will still require investments to improve their health care infrastructure.
New York can ensure that the community-level health care infrastructure needs of racial, ethnic, and language minority patients are better addressed by:
Supporting “safety net” hospitals and community health centers, and reducing the financial vulnerability of health care institutions serving poor and minority communities
People of color, immigrants and low-income individuals are more likely than other populations to access health care in safety net institutions, such as public hospitals and community health centers.41 In many cases, these institutions face financial vulnerability because of low Medicaid reimbursement rates and/or the costs of providing uncompensated care to uninsured individuals.42 These institutions may fare better in states where near-universal health insurance coverage proposals are enacted and where health insurance expansions are realized, but they will likely continue to face financial vulnerability until universal and equitable coverage is achieved.
New York operates a free care/bad debt pool aimed at reimbursing hospitals for uncompensated care. Yet the U.S. Department of Health and Human Services has said that many of New York’s most financially troubled hospitals will go bankrupt or default on their loans without more state assistance.43 State health care expansion proposals should include provisions to provide additional financial resources or other support to safety net institutions, particularly until coverage plans “ramp up” to reach uninsured populations. The viability of these institutions is particularly important if New York fails to establish truly “universal” coverage due to exclusion of childless adults or undocumented immigrants who are not eligible for Medicaid and are subject to enrollment caps in many state-funded programs—exclusions which we recommend against. In such a scenario, New York would likely rely on safety net institutions to provide a significant uninsured population with primary and preventative health care that is essential to the state’s health.
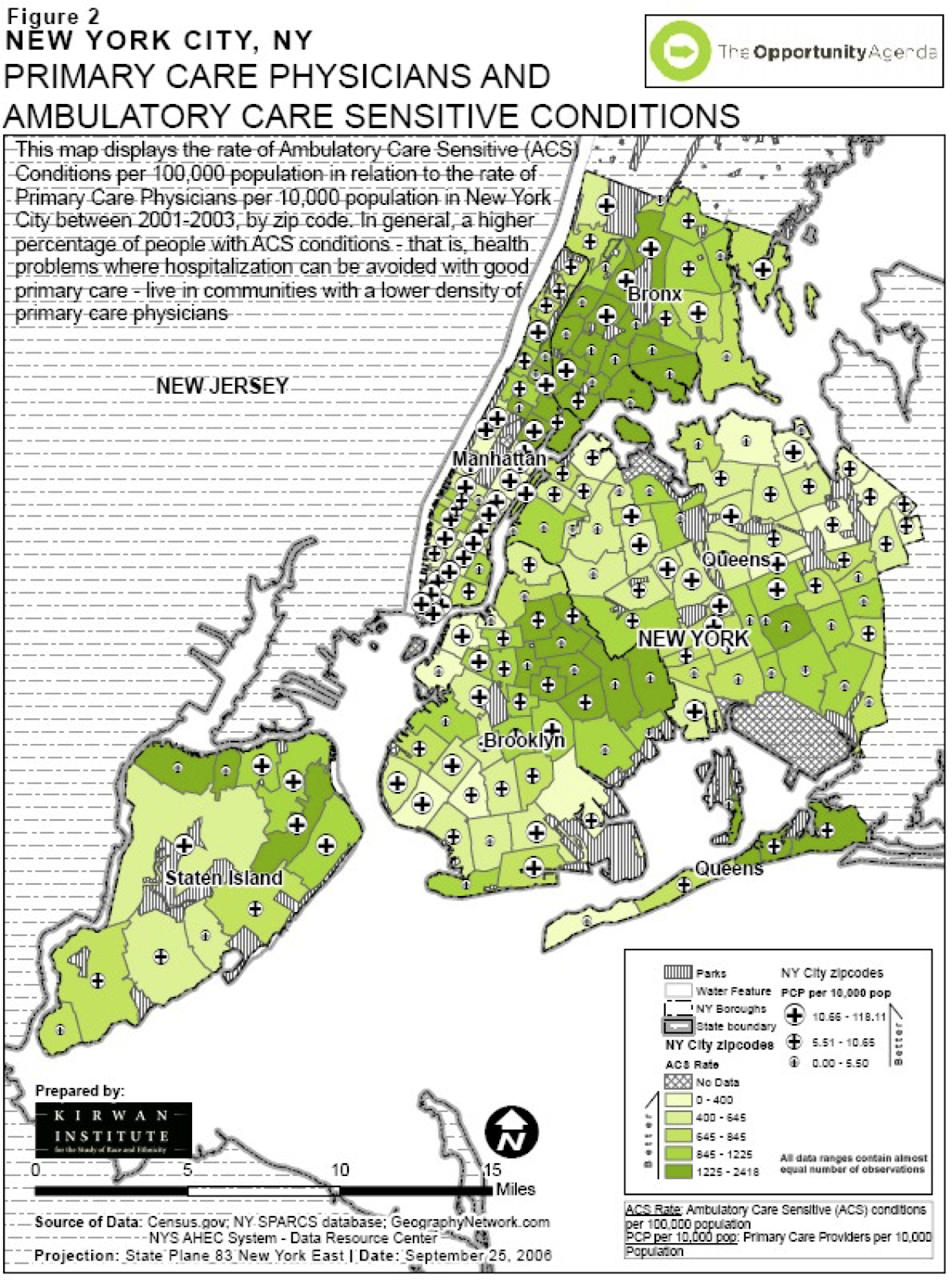
Creating and/or improving incentives for health care professionals to practice in underserved communities
Low-income and minority communities often have the most pressing need for health care services, but they are served by a dwindling number of providers and institutions that lack resources to expand and improve services (Figure 2).44 New York can address this imbalance by providing incentives, such as funds for graduate medical education programs that focus on underserved populations, tuition reimbursement and loan forgiveness programs that require service in communities with health professional shortage areas.
V. State Program and Policy Infrastructure
New York can improve its capacity to plan for and address the health care policy challenges and needs of minority communities by adopting or strengthening existing policies such as:
Community health planning
Community health planning is a means of gaining community input and better aligning health care resources with community needs. Community health planning has a long history, but its promise as a tool to reduce health care disparities has yet to be fully realized. Community health planning seeks to strengthen communities to play a greater role in their own health, actively involving residents in the planning, evaluation, and implementation of health activities in their communities. The 1974 National Health Planning Law sought to create and support a network of community Health Systems Agencies (HSAs), but a lack of funding and effective mechanisms for community input to shape health policy has led to a decline of HSA power and influence.45
In New York, the laws creating a statewide Health Systems Agency remain on the books,46 though the State stopped funding the agency in the 1990s.47 Despite its decline, HSAs have been proven effective and significant tools for equity in New York. The Finger Lakes HAS (FLHSA), for example, has served as an important vehicle to address the common concerns of consumer groups, businesses, health plans, and providers regarding health planning.48 Through collaboration between the Rochester community, local businesses, and the local insurer, Blue Cross Blue Shield, FLHSA has remained an active, self-funded project, but requires greater funding support to remain a broad-based planning agency. New York can integrate strategies to restart and reinvigorate HSAs and include disparities reduction efforts as part of the mission of these planning agencies into its health care expansion proposals.
Certificate of Need assessment
Historically, the purpose of the Certificate of Need (CoN) process has been to control health care costs and ensure that capital and technology investments in the health care industry reflect community needs. In New York, the process has required hospitals and other health care institutions that seek to establish, expand or reduce services to submit proposals so that the Department of Health can evaluate projects to eliminate unnecessary duplication of services and ensure that investments strategically address health care needs. The CoN process, however, has great potential to encourage a better distribution of health care resources, reflecting community and statewide need.49 The four current criteria examined by the DOH through the CoN—public need, financial feasibility, character/competence and construction50—are necessary but insufficient to ensure reflection of community needs. Although DOH is required to assess public need in determining whether to grant a Certificate of Need application for the construction, expansion, or conversion of hospitals,51 the agency has not historically done so (Figure 3).52 New York should re-evaluate and reinvigorate the CoN process through new policies that ensure accountability for the use of public funds; reduce geographic, racial, ethnic and socioeconomic disparities; and reduce the “fragmentation” of the health insurance market. Specifically, New York should ensure that the collection of data revealing racial/ethnic, language status, and income-based health care disparities, discussed above, is integrated into the CoN process. DOH should make obtaining a Certificate of Need contingent on evidence that changes sought would reduce racial and economic health care inequality.53
Figure 3
Coordination between DOH, DOI, the New York State Division of Human Rights, and the Attorney General
The New York State Division of Human Rights is charged with reviewing complaints under the New York State Human Rights Law and enforcing the law. However, few complaints reviewed by the State Division address discrimination in access to health care.54 But because discrimination in health care is often covert, structural, and sometimes unintentional, review of these limited number of complaints are not alone a good way to discover and eliminate existing racial discrimination. The State Division should exercise its power to initiate its own investigations, file its own complaints, and conduct studies in compliance with state, federal and international human rights law and to prevent and eliminate discrimination in access to health care.55
To this end, New York should develop a comprehensive, statewide approach to eliminating racial and ethnic health disparities, grounded in the fundamental understanding that these disparities stem from historical, interpersonal and institutional racism. The State is empowered to eliminate health care gaps through its control of funding, power of regulation and control over the authorization of hospital closings and downsizing to control the allocation of health care resources. Moreover, the Attorney General possesses broad authority under parens patriae standing, which provides states with the ability to sue to protect the health of their residents.56 The Departments of Health and Insurance, the Office of the Attorney General, and the State Division of Human Rights should coordinate efforts to end health disparities based on race or ethnicity. One model of coordination is a bill pending before the Massachusetts legislature to establish an Office of Health Equity to coordinate all efforts to eliminate racial and ethnic discrimination in health care.57 An equally comprehensive government-led initiative in New York would need: (1) to share the honesty of the Massachusetts Commission to End Racial and
Ethnic Health Disparities58 in acknowledging that racial and ethnic health disparities are caused by racism and institutional tolerance of racial bias; (2) to be led by influential policymakers who could implement the recommendations into law; and (3) to examine and address the multiple causes of disparities, including health care services, patient education and behavior, and larger social conditions.59
VI. Policies to Address Social and Community-Level Determinants of Health
While largely outside of the purview of state health insurance coverage expansion proposals, any effort to reduce racial and ethnic health status gaps must address factors that lie largely outside of the health care arena. These include social and community-level determinants of health—such as environmental conditions in homes, employment, or educational institutions—which are powerful “upstream” predictors of who is healthy and who is ill. New York State health care reform proposals can consider strategies to:
Improve coordination of relevant state agencies that should address determinants (e.g., education, housing, employment)
State agencies that seek to reduce social and economic gaps are inherently engaging in health equity work. Almost all aspects of state policy in education, transportation, housing, commerce, and criminal justice influence the health of state residents, and can have a disproportionate impact on underserved communities. New York can take steps to coordinate the work of state agencies that impact health disparities, which would likely reduce duplication of effort, increase efficiency, and more effectively address health outcome disparities.
Health impact assessment (HIA) policies
HIA attempts to ensure that all government programs and initiatives in and outside of the health care delivery sector—such as transportation, housing, and environmental protection—are assessed to determine their potential impact on the health status of affected communities.60 HIA is used extensively as a policy and planning tool in Europe and other countries, and is used increasingly in the United States. The San Francisco Department of Public Health, for example, has developed and implemented the Healthy Development Measurement Tool to identify and assess community health needs and understand how land use and development projects can complement public health goals. New York should determine whether state health care expansion proposals include use of health impact assessments to assist planning.
Conclusion
New York is synonymous with opportunity in the American vocabulary. In considering health care system proposals, we ask that you evaluate not only whether a greater number of residents will be insured, but also whether system reform proposals improve the equal opportunity of New York residents to access quality health care. We hope the equity benchmarks laid out above will assist in your evaluation process.
Notes:
1. N.Y. CONST. art. XVII, §§ 1, 3.
2. Civil Rights Act of 1964, tit. VI, 42 U.S.C. §2000d et seq.; Civil Rights Act of 1964, tit. VII, 42 U.S.C. §2000e et seq.; Nondiscrimintion Under Programs Receiving Federal Assistance Through the Department of Health and Human Services Effectuation of Title VI of the Civil Rights Act of 1964, 45 C.F.R. §80.3 (2005); Guidance to Federal Financial Recipients Regarding Title VI Prohibition Against National Origin Discrimination Affecting Limited English Proficient Persons, 68 Fed. Reg. 47311 (2003)
2. International Convention on the Elimination of All Forms of Racial Discrimination, Dec. 21, 1965, 140 CONG. REC. 14326, 660 U.N.T.S. 195.
3. Medicaid Act, Pub. L. No. 89-97, tit. I, 79 Stat. 343 (1967); Hospital Survey and Construction Act (“Hill-Burton Act”), Pub. L. No. 88-443, 78 Stat. 447, 42 U.S.C. §§ 291-291(o) (1964).
4. Poll designed by Harvard School of Public Health and conducted by The Opportunity Agenda from October 24th to November 13th, 2006, with a representative sample of 479 New York State residents over the age of 18. The margin of error is +/-4.48% at the 95% confidence level.
5. N.Y. CONST. art. XVII, §3.
6. N.Y. CONST. art. XVII, §3. The text of the public health provision makes clear that it covers both the “protection” and the “promotion” of health, that it covers all “inhabitants” of the State, and that provision for such protection and promotion by state and municipal governments is mandatory. Courts have generally found that use of the term “shall” establishes a mandate. See, e.g., Nat’l Ass’n of Home Builders v. Defenders of Wildlife, 127 S. Ct. 2518, 2531-32 (2007) (finding the statutory language “shall approve” mandatory) (citing Lopez v. Davis, 531 U.S. 230, 241 (2001) (noting Congress'”use of a mandatory ‘shall’ . . . to impose discretionless obligations”); Lexecon Inc. v. Milberg Weiss Bershad Hynes & Lerach, 523 U.S. 26, 35 (1998) (“The mandatory ‘shall’ . . . normally creates an obligation impervious to judicial discretion”); Association of Civil Technicians v. FLRA, 22 F.3d 1150, 1153 (D.C. Cir. 1994) (“The word ‘shall’ generally indicates a command that admits of no discretion on the part of the person instructed to carry out the directive”); Black’s Law Dictionary 1375 (6th ed. 1990) (explaining that “[a]s used in statutes . . . this word is generally imperative or mandatory” and noting that in legal documents “shall” is construed as permissive only when necessary to carry out legislative intent or in cases where no right depends on its being taken in a mandatory sense). As the section of the state constitution on state finance explains: “Subject to the limitations on indebtedness and taxation, nothing in this constitution contained shall prevent the legislature from providing . . . for the protection by insurance or otherwise, against the hazards of unemployment, sickness and old age.” NY CONST. art. VII § 8.
7. STATE COVERAGE INITIATIVES & ACADEMY HEALTH, STATE OF THE STATES: BUILDING HOPE AND RAISING EXPECTATIONS (2007).
8. Supra note 4.
9. INST. OF MEDICINE, CROSSING THE QUALITY CHASM: A NEW HEALTH SYSTEM FOR THE 21ST CENTURY (2001).
10. INST. OF MEDICINE, UNEQUAL TREATMENT: CONFRONTING RACIAL AND ETHNIC DISPARITIES IN HEALTH CARE (2003).
11. THE OPPORTUNITY AGENDA, DANGEROUS AND UNLAWFUL: WHY OUR HEALTH CARE SYSTEM IS FAILING NEW YORK AND HOW TO FIX IT 42 (2006), available here.
12. Id. at 4.
13. Id.
14. U.S. CENSUS BUREAU, INCOME, POVERTY, AND HEALTH INSURANCE COVERAGE IN THE US: 2006 (2007).
15. D. HOLAHAN ET AL., UNITED HOSPITAL FUND, HEATH INSURANCE COVERAGE IN NEW YORK, 2001 (2003).
16. THE OPPORTUNITY AGENDA, DANGEROUS AND UNLAWFUL, supra note 11.
17. INST. OF MEDICINE, UNEQUAL TREATMENT, supra note 10.
18. Id..
19. See, e.g., M.M. Doty & A.L. Holmgren, Health care disconnect: gaps in coverage and care for minority adults. Findings from the Commonwealth Fund Biennial Health Insurance Survey, 2005 (Commonwealth Fund, Issue Brief, 2006); J.L. Hargraves & J. Hadley, The contribution of insurance coverage and community resources to reducing racial/ethnic disparities in access to care, 38 HEALTH SERVS. RESEARCH 809, 809-29 (2003); M. Lillie-Blanton & C. Hoffman, The role of health insurance coverage in reducing racial/ethnic disparities in health care, 24 HEALTH AFFAIRS 398, 398-408 (2005); R.M. Weinick et al., Who can’t pay for health care?, 20 J. OF GEN. INTERNAL MED. 504, 504-09 (2005).
20. MELVIN L. OLIVER & THOMAS M. SHAPIRO, BLACK WEALTH, WHITE WEALTH (1997).
21. Kathryn Pitkin Derose et al., Immigrants and Health Care: Sources of Vulnerability, 26 Health Affairs 1285, 1258-68 (2007).
22. C. Brach & I. Fraser, Reducing disparities through culturally competent health care: an analysis of the business case, 10(4) QUALITY MGMT. IN HEALTH CARE 15-28 (2002).
23. OFFICE OF MINORITY HEALTH, U.S. DEP’T OF HEALTH & HUMAN SERVS., NATIONAL STANDARDS FOR CULTURALLY AND LINGUISTICALLY APPROPRIATE SERVICES IN HEALTH CARE.
24. Id. at 10-13. All recipients of federal funds are mandated to meet Standards 4, 5, 6, and 7, which are based on Title VI of the Civil Rights Act as applied to Limited English Proficiency (LEP) persons. Standard 4 requires provision of bilingual staff and interpreter services at all hours to LEP persons. Standard 5 requires provision of oral offers and written notices to patients, in their preferred language, of their right to receive language assistance services. Standard 6 requires competence of language service providers and discourages the use of friends or family. Standard 7 requires materials and signage posted in the service area in languages of commonly encountered language populations.
25. INST. OF MEDICINE, IN THE NATION’S COMPELLING INTEREST: ENSURING DIVERSITY IN THE HEALTH CARE WORKFORCE (2004).
26. S.L Taylor & N. Lurie, The role of culturally competent communication in reducing ethnic and racial healthcare disparities, 10 AM. J. OF MANAGED CARE Spec. No.:SP1-4 (2004)
27. INST. OF MEDICINE, UNEQUAL TREATMENT (2003).
28. Cal. AB 8, 2007-08 Reg. Sess., § 1366.10 (2007).
29. C. Brach et al., Who’s enrolled in the State Children’s Health Insurance Program (SCHIP)? An overview of findings from the Child Health Insurance Research Initiative (CHIRI), 112 PEDIATRICS e499 (2003); D.C. Ross & I.T. Hill, Enrolling eligible children and keeping them enrolled, 13 FUTURE CHILD 81, 81-97 (2003); M.C. Morreale & A. English, Eligibility and enrollment of adolescents in Medicaid and SCHIP: recent progress, current challenges, 32 J. OF ADOLESCENT HEALTH 25, 25-39 (2003).
30. L.P. Shone et al., The role of race and ethnicity in the State Children’s Health Insurance Program (SCHIP) in four states: are there baseline disparities, and what do they mean for SCHIP?, 112 PEDIATRICS e521 (2003).
31. R.T. Perot & M. Youdelman, Racial, ethnic and primary language data collection in the health care system: An assessment of federal policies and practices (Commonwealth Fund, Commonwealth Fund Publication No. 492, Sept. 2001). S.D. Watson, Equity measures and systems reform as tools for reducing racial and ethnic disparities in health care (Commonwealth Fund, Commonwealth Fund Publication No. 776, Aug. 2005).
32. R.T. Perot & M. Youdelman, supra note 21; INST. OF MEDICINE, UNEQUAL TREATMENT (2003).
33. P.L. Casalino & A. Elster, Will Pay-For-Performance and quality reporting affect health care disparities?, 26 HEALTH AFFAIRS w405-14; R.G. Hood, Pay-For-Performance—Financial Health Disparities and the Impact on Healthcare Disparities, 99 J. OF THE NAT’L MED. ASS’N 953, 953-58 (2007).
34. INST. OF MEDICINE, UNEQUAL TREATMENT (2003).
35. D. Kalauokalani et al., Can patient coaching reduce racial/ethnic disparities in cancer pain control? Secondary analysis of a randomized controlled trial, 8 PAIN MED. 17, 17-24 (2007).
36. INST. OF MEDICINE, UNEQUAL TREATMENT (2003).
37. H.P. Freeman, Patient navigation: a community centered approach to reducing cancer mortality, 21 J. CANCER EDUC. Suppl. S11, S11-14 (2006); M.L. Steinberg et al., Lay patient navigator program implementation for equal access to cancer care and clinical trials: essential steps and initial challenges, 107 Cancer 2669, 2669-77 (2006). 38 N.Y. State Dep’t of Health, Community Health Worker Program.
39. COMMUNITY VOICES, COMMUNITY HEALTH WORKERS AND COMMUNITY VOICES: PROMOTING GOOD HEALTH (2003).
40. Id. at 13-14.
41. Kaiser Comm’n on Medicaid & the Uninsured, Stresses to the Safety Net: The Public Hospital Perspective, June 2005; J. Hadley et al., Would safety- net expansions offset reduced access resulting from lost insurance coverage? Race/Ethnicity differences, 25 HEALTH AFFAIRS 1679 (2006). Also note that New York provides Medicaid coverage to eligible documented immigrants, increasing the importance of safety-net institutions for many New Yorkers. Aliessa v. Novello, 96 N.Y.2d 418 (2001).
42. D.P. Andrulis, L.M. Duchon, SUNY Downstate Med. Ctr., Hospital care in the 100 largest cities and their suburbs, 1996-2002: Implications for the future of the hospital safety net in metropolitan America, Aug. 2005.
43. HHS was called the “Department of Housing and Urban Development” at the time of the statement. N.Y. State Assembly, Press Release, Health Care Reform Act of 2000 (1999).
44. P. Cunningham, Mounting pressures: physicians serving Medicaid patients and the uninsured, 1997-2001 (Center for Studying Health System Change, Tracking Report No. 6, Dec. 2002); P. Cunningham & J. May, Medicaid patients increasingly concentrated among physicians (Center for Study Health System Change, Tracking Report No. 16, Aug. 2006).
45. D.A. Conrad, Community care networks: linking vision to outcomes for community health improvement, 60 MED. CARE: RESEARCH & REV. Suppl. 95, 95-129 (2003); S. Sofaer, Community health planning in the United States: a postmortem, 10(4) FAMILY & COMMUNITY HEALTH 1, 1-12 (1988); R. Weech-Maldonado et al., Evaluating the effectiveness of community health partnerships: a stakeholder accountability approach, 26 J. OF HEALTH & HUMAN SERVS. ADMIN. 58, 58-92 (2003); L.B. LANDRUM, HEALTH PLANNING IS ALIVE AND WELL, AM. HEALTH PLANNING ASS’N.
46. N.Y. PUB. HEALTH § 2904-b.
47. Calling Upon the Legislature of the State of New York to Amend the Health Care Reform Act to Reauthorize Funding for Health Systems Agencies (Mar. 24, 1998); Judy Wessler, Comm’n on the Public’s Health System, Press Advisory, The Need for Health Planning (undated; on file with Judy Wessler, Comm’n on the Public’s Health System).
48. See Finger Lakes Health Systems Agency, Current Projects.
49. D.B. Smith, Eliminating Disparities in Treatment (Commonwealth Fund, Aug. 2005).
50. Public need considers the hospital’s impact on the specific population demographic regarding access to specific health services, facility utilization patterns and how the hospital will affect the epidemiology of certain relevant diseases in the community. Financial feasibility examines the hospital’s financial health, projected costs and potential profits/expenses regarding the specific project. Character/competence examines the hospital’s prior experience and success in operating a healthcare facility. Finally, construction deals with the hospital’s adherence to pertinent New York State regulations regarding the building of healthcare facilities.
51. In determining whether an application for construction, expansion, conversion should be granted, DOH is required to consider public need, as well as financial feasibility, character and competence, and construction. In determining whether to revoke an operating certificate, DOH is also required to consider public need; but in its approval of voluntary closures DOH has argued that it need not consider health needs. See N.Y. State Dep’t of Health, Certificate of Need Review Criteria.
52. In the mid-1980s, in response to a Title VI complaint filed by Legal Services of New York and New York Lawyers for the Public Interest, DOH entered negotiations with advocates and agreed to add a form to its Certificate of Need application that would address concerns about access to health care. Telephone interview with Judy Wessler, Director, Commission on the Public’s Health System (Nov. 16, 2006). The form, at the time identified as Schedule 18, required health care facilities to address access to facilities, including language access, in their applications and obligated DOH to weigh such issues in deciding whether to approve applications. Id. Schedule 18 no longer addresses health care access issues; it now applies to Residential Health Care Facilities. N.Y. State Dep’t of Health, Schedule 16 – CON Forms Specific to Residential Health Care Facilities. But this requirement was only enforced for a short time, while legal and community groups reviewed DOH procedures. The parts of the current Certificate of Need application that address issues of access and public need must once again be reviewed and enforced. A specific schedule is designated for each Article 28 facility. Schedule 16 applies to hospitals and Schedule 17 applies to Diagnostic and Treatment Center. N.Y. State Dep’t of Health, Schedule 16 – CON Forms Specific to Hospitals; N.Y. State Dep’t of Health, Schedule 16 – CON Forms Specific to Diagnostic and Treatment Centers (D&TC). Only Schedule 16 appears to require a facility access analysis for hospitals. See N.Y. State Dep’t of Health, Schedule 16 – CON Forms Specific to Hospitals, supra.
53. DAVID BARTON SMITH, ELIMINATING DISPARITIES IN TREATMENT AND THE STRUGGLE TO END SEGREGATION
(2005) (“Currently, specialized services such as open-heart surgery are moving from the inner suburbs of most urban areas to the outer ones, following white flight and urban sprawl. Market and convenience justifications mask a resegregation of care that increases the cost of health care and reduces its quality.”).
54. In Fiscal Year 2002-2003 only 2.8% of the complaints filed with the State Division complained of discrimination in public accommodations; in Fiscal Year 2003-2004, the number increased slightly to 3.1%. N.Y. State Div. of Human Rights, Annual Report, Website Ed., Fiscal Years 2002/2003-2003/2004.
55. The Division is empowered to develop human rights plans and policies for the state and to assist in their execution. The Division may convene “advisory councils, local, regional or state-wide . . . to study the problems of discrimination in all or specific fields of human relationships or . . . specific instances of discrimination because of age, race, creed, color, national origin, sexual orientation, military status, sex, disability[,] or marital status and [to] make recommendations to the division for the development of policies and procedures.” N.Y. EXEC. LAW § 295(8) (2006); see also N.Y. EXEC. LAW § 295(6)(b) (2006); N.Y. EXEC. LAW § 295(9) (2006); 18 N.Y. JUR. CIV. RTS. § 14 (2006).
56. DENNIS D. PARKER, STATE REFORM STRATEGIES, IN AWAKENING FROM THE DREAM 317, 322 (Denise Morgan, et al., eds., 2006). States have brought civil rights cases alleging discrimination in housing, public accommodations, access to health care, and employment, under parens patrie standing.
57. H. 2234, 185th Gen. Court (Ma. 2007).
58. A 3-year project that brought together legislators, community members, and experts in health and health care. Comm’n to End Racial & Ethnic Health Disparities, Final Report (Aug. 2007).
59. Id.
60. A.L. Dannenberg et al., Growing the field of health impact assessment in the United States: an agenda for research and practice, 96 Am. J. of Public Healt 262, 262-70 (2006).
