Welcoming a baby into the world should be a time of joy and excitement. But for many Black mothers in the United States, childbirth is a milestone where racial stereotypes, systemic racism, and healthcare inequities collide, leading to disparate and harmful outcomes and experiences.
The United States is the only industrialized nation in the world where maternal mortality is rising. Black women are three to five times more likely to die from pregnancy complications than white women[1], and 80 percent of those deaths are preventable.[2] Similarly, relative to other infants, Black infants are more than twice as likely to die before their first birthday.[3] If the health of a society can be measured by its maternal and infant mortality rates, the United States is failing.
Women in the Room Productions’ documentary, Birthing Justice, addresses this national crisis by turning the spotlight on the progress being made by health initiatives and uplifting evidence-based practices to adopt more widely. With input from advocates and leaders in the birthing justice movement, the film offers solutions that can be implemented in communities across the country. From supporting Black doulas and midwives to embracing practices that ensure Black mothers are heard and listened to, the film directs viewers to solutions for reproductive justice.
SOCIAL ISSUE BACKGROUND
The color of one’s skin should not determine the quality of healthcare a woman receives during pregnancy. Yet the following statistics show how interpersonal racism and implicit bias – along with structural racism – have tragically led to substandard healthcare for Black mothers in the United States:
Black women are three to five times more likely to die from pregnancy complications than white women.
Preeclampsia/eclampsia is the leading cause of maternal death among Black women.[4]
Black mothers experience stillbirths at double the rate of white mothers.[5]
Black infants die at two to three times the rate of white infants.
These discrepancies persist regardless of a mother’s socioeconomic status or education. Changes to the system can help dramatically. For example, when Black babies are delivered by Black doctors, their mortality rate is cut in half.[6] Developing pathways to diversify clinical care teams, specifically training and investing in Black providers in the healthcare system, are what Birthing Justice and The Opportunity Agenda are advocating for.
When watching Birthing Justice, we encourage you to consider the courage and resilience of the interviewees sharing their stories. The documentary follows Black women through pregnancy, delivery, and the postpartum period—exposing the challenges Black mothers encounter, including genetic predispositions, chronic stress, racial bias, disrespectful care, and barriers to adequate healthcare.
Historically, the narrative around the Black/white disparity in infant mortality placed the blame on Black mothers. In fact, investigations conducted more than two decades ago revealed the racist diagnosis accepted by medical professionals that poor, less-educated women of color put their lives and the lives of their children at risk by smoking, drinking, using drugs, and not eating right.[7] It was also unbelievably speculated that Black mothers should be held responsible for their pregnancy losses (including miscarriages and stillbirths) if they were too young, unmarried, or didn’t seek medical help during and after their pregnancies.
Birthing Justice disproves these harmful narratives, revealing how inequitable systems and structures have resulted in racial injustices in maternal and infant health. The film shows how we can come together to end this national tragedy by supporting policy solutions that provide Black mothers with resources that allow them to make informed decisions for themselves and their families.
We encourage you to consider the courage and resilience of the interviewees sharing their stories.
DISCUSSION BACKGROUND
Admittedly, it can be very uncomfortable to have discussions about mortality, racism, and reproductive health. Many of us may feel defensive or not heard when we have these conversations. We understand that.
We also know that open and respectful dialogue allows us to grow as individuals and as a community. Most people have long held and often distorted views about race, racism, mothers, and Black women, so it is important to be open to hearing different perspectives and experiences.
As community members, we share many of the same values: family, health, fairness, and justice. A willingness to have these uncomfortable conversations ensures that everyone experiences the ideals behind these values. We encourage you to enter the discussion about Birthing Justice with an open mind and an eagerness to share your experiences with others who may benefit from watching the film.
We want to acknowledge that the film presents sensitive subject matter, particularly for those who have experienced birth trauma and their families.
DISCUSSION QUESTIONS
How did the film challenge your previously held perceptions about Black mothers, reproductive health, or the medical industry?
What kinds of stereotypes or media representations have you seen about Black mothers before watching Birthing Justice?
How do you think those stereotypes and/or media representations have impacted the outcomes discussed in the film?
Were you surprised to learn that all Black mothers, including well-educated and financially secure ones, and even famous women, can experience racism in maternal health?
Why do you think there is unequal access to medical services? How might the history of the medical profession and systemic racism explain these inequities?
How do you think we can eliminate bias in our healthcare system?
What are ways that health care institutions can be held accountable in providing Black women and birthing people with respectful maternity care?
What do you think the impact of anti-abortion laws will be on people who are living in poverty? How do you think we should prepare medical professionals for these situations?
How might you support Black women and birthing people in accessing resources about midwives, doulas, and other providers who embrace holistic healthcare practices?
PERSONAL REFLECTION
I relate most with [someone from film] . . .
This documentary made me feel . . .
Healthcare in this country should be . . .
Black women and birthing people deserve . . .
It is important to also discuss legislative solutions for our nation’s Black maternal health crisis. For example, members of Congress have been considering a 12-month postpartum Medicaid coverage package that would offer significant support to low-income Black mothers. This, along with the Black Maternal Health Momnibus Act, would provide essential coverage for Black birthing people.
When it comes to finding systemic solutions, we believe that government plays a role. In addition to federal policies, there may also be local legislation on the books in your state to address the crisis. We encourage you to reach out to the following advocacy groups to get involved:
GET INVOLVED
Many organizations are working to improve Black maternal health outcomes. You can support and invest in these national and local groups through donations, by following them on social media, or by sharing information about them with others in your network.
Birth Injury Center
Birth injuries can transform the celebratory moment of a child’s birth into a lifelong nightmare that includes serious health complications, permanent disability, or death. The Birth Injury Center provides support and resources to families impacted by birth trauma.
Black Mamas Matter Alliance (BMMA)
A national network of Black women-led and Black-led birth and reproductive justice organizations and multidisciplinary professionals who work across the full spectrum of maternal and reproductive health.
Black Maternal Heath Caucus
Launched by Congresswomen Alma Adams and Lauren Underwood, this caucus is dedicated to elevating the Black maternal health crisis within Congress and advancing policy solutions to improve Black maternal health outcomes and end disparities.
Black Women Birthing Justice
A grassroots collective of Black women and individuals across the African diaspora committed to transforming birthing experiences for Black women and birthing people.
Black Women for Wellness
An organization committed to the health and well-being of Black women and girls through health education, empowerment, and advocacy.
Center for Black Women’s Wellness
A premier, community-based, family service center committed to improving the health and well-being of underserved Black women and their families.
Community of Hope’s Family Health and Birth Center
This facility includes a nationally accredited Birth Center and provides a range of healthcare services for entire families, with a special focus on serving pregnant parents and their babies.
Every Mother Counts (EMC)
EMC works to make pregnancy and childbirth safe for every mother, everywhere, by raising awareness, investing in solutions, and mobilizing action.
Moms Rising
A network of people taking on the most critical issues facing women, mothers, and families, as well as educating the public and mobilizing grassroots action to build a more family-friendly America.
National Black Equity Collaborative (NBEC)
NBEC works for birth equity for all Black birthing people, with a willingness to address racial and social inequities in a sustained effort.
SisterSong Women of Color Reproductive Justice Collective
This organization is dedicated to building an effective network of individuals and organizations to improve institutional policies and systems that impact the reproductive health of Black women.
ADDITIONAL RESOURCES
To learn more about Black maternal health:
Battling Over Birth: Black Women and the Maternal Health Care Crisis in California
By Chinyere Oparah, Linda Jones, Dantia Hudson, Talita Oseguera, and Helen Arega
This book documents the Black maternal health crisis and aims to ensure that every Black mother has an empowered birthing experience.
Implicit Bias Test
Founded in 1998, Project Implicit educates the public about their personal hidden biases and brings them to light through an online “virtual laboratory.”
Birthing Justice: Black Women, Pregnancy, and Childbirth
Edited by Julia Chinyere Oparah and Alicia D. Bonaparte
This book places Black women’s voices at the center of the debate on what should be done to fix the broken maternity system. It also foregrounds Black women’s agency in the emerging birth justice movement. Mixing scholarly, activist, and personal perspectives, the book shows readers how they, too, can change lives — one birth at a time.
ACKNOWLEDGEMENTS
Special thanks to Denise Pines, I. India Thusi, Rahel Samantrai, Abby Akrong, Elizabeth Johnsen, Julie Fisher-Rowe, Cecilia Martinez, J. Rachel Reyes, Ellen Buchman, Isabel Morgan, and Lorissa Shepstone.
Women in the Room Productions is a comprehensive media company that drives social impact for women and persons of color through storytelling and community.
The Opportunity Agenda builds the public imagination and cultural will to challenge white supremacy. We advance narratives that support opportunity for all and work in community with partners to overcome opposition narratives that exclude and divide us. www.opportunityagenda.org
CITATIONS
1 Marian F. MacDorman Marie Thoma, Eugene Declcerq, & Elizabeth A. Howell, Racial and Ethnic Disparities in Maternal Mortality in the United States Using Enhanced Vital Records, 2016-17, 111 Am. J. Pub. Health 1673 (2021).
3 Ely DM, Driscoll AK. Infant mortality in the United States, 2020: Data from the period linked birth/infant death file. National Vital Statistics Reports; vol 71 no 5. Hyattsville, MD: National Center for Health Statistics. 2022. DOI: https://dx.doi. org/10.15620/cdc:120700.
6 Greenwood BN, Hardeman RR, Huang L, Sojourner A. Physician-patient racial concordance and disparities in birthing mortality for newborns. Proc Natl Acad Sci U S A. 2020 Sep 1;117(35):21194-21200. doi: 10.1073/pnas.1913405117. Epub 2020 Aug 17. PMID: 32817561
7 PH Wise & DM Pursley, Infant Mortality as a Social Mirror.
Today, the United States Supreme Court took the dreaded step to overrule Roe v. Wade and Planned Parenthood v. Casey with its decision in Dobbs v. Jackson Women’s Health. The Court has now restricted the right of hundreds of millions of Americans to decide for themselves whether to have an abortion, uprooting decades of precedent and a right upon which hundreds of thousands of Americans have relied.
While today is a tremendous setback and sad day for our country, it is important to remain vigilant in the fight for social justice and bodily autonomy when communicating about Dobbs. While it is tempting to focus only on the sadness of the day, we must stick together and clarify in our communications that we will not stop pushing forward toward justice until full rights are realized for everyone.
We recognize that this opinion not only threatens reproductive freedom for millions, but that the Court’s inconsistent contemplation of whether a right even exists could jeopardize other rights. This may include the rights of people in same-sex relationships and interracial relationships, and the right to use contraceptives. Therefore, it is critical to advance a narrative that recognizes the aspiration of full rights and justice and the inherent values at stake in this decision, including:
Dignity;
Equal Justice; and
Freedom
We recommend bringing a values-focused framework when talking about this issue and focusing on solutions rather than on only the problems or the sadness of the day.
Key Takeaways
Dobbs represents a fundamental threat to reproductive liberty and justice.
Dobbs allows states to take action by banning any and all access to abortion. Less than one hour after the Court announced its decision in Dobbs, the state of Missouri’s attorney general swiftly implemented that state’s abortion ban. More than 25 states will likely take action to eliminate nearly all abortion rights immediately.[1] Even outside of the states considering complete bans, abortion rights may be severely weakened.
The repercussions could mean enhanced discrimination, forcing people without economic means, especially people of color, to travel extensively outside of the state they live in to have an abortion. As a result, the poorest Americans without financial resources to travel will face the brunt of having their reproductive liberty being stripped away.
Communicate that Dobbs will have a detrimental impact on the reproductive freedom, health, and dignity of millions of people across the country – especially low-income women and people of color.
Dobbs opens the door to weaken or eliminate many other fundamental rights.
In addition to how personhood is defined and whether fetuses should have the same rights as people, there are many other implications to the Dobbs ruling. Reproductive justice is not the only right that may be impacted. The Court’s narrow construction of the right to abortion in Dobbs comes from its reliance on Washington v. Glucksberg, in which the Court reconstrues Glucksberg to narrowly evaluate whether a right is protected. It asks whether that specific right is “deeply rooted in this nation’s history and tradition.” This means that instead of asking whether the right to privacy protects a specific right, courts can now ask whether that specific right, e.g. the right to buy contraception, was traditionally protected in the eighteenth century. This is a very narrow approach, which can be contrasted by the Supreme Court’s approach to marriage equality in Obergefell v. Hodges.
In Obergefell, the Court recognized a right for same-sex couples to get married and noted that the Glucksberg approach was overly narrow. It said that the proper approach is to ask whether the constitutional right to privacy meant that same-sex partners should be allowed to marry. The Court’s method for interpreting whether a right exists in Dobbs means that many other rights are at risk. This method could result in the erosion of freedoms, from the right to same-sex and interracial marriage, to the right to use contraceptives.
Right-wing activists and lawyers are already planning their assault on a broader set of rights. For example, Jonathan Mitchell, the former Solicitor General of Texas and the architect of Texas’s notorious SB-8 law, which restricts access to abortions, argued in an amicus brief that the logic to overrule Roe could be used to overrule Lawrence v. Texas and Obergefell v. Hodges:
“This is not to say that the Court should announce the overruling of Lawrence and Obergefell if it decides to overrule Roe and Casey in this case. But neither should the Court hesitate to write an opinion that leaves those decisions hanging by a thread. Lawrence and Obergefell, while far less hazardous to human life, are as lawless as Roe.”[2]
The Dobbs opinion overruled a watershed precedent, weakening the Court’s legitimacy.
Dobbs overruled Roe v. Wade, which had been the law of the land for nearly 50 years. The principle of stare decisis, that a court respects and gives deference to decisions before it, is crucial in preserving the legitimacy of the Court. At his nomination hearing, Justice Alito himself stated that stare decisis was “a fundamental part of our legal system” despite his blatant disregard for the principle in Dobbs.[3]
Public polling has shown that the Court’s support dropped significantly in the wake of the leaked draft opinion of Dobbs, which greatly resembles the final version.[4]
Emphasize how the Court has significantly undermined its own legitimacy by ignoring its own precedent.
Key Questions
Some people say that this case is only about abortion and people who say otherwise are being alarmist. How should advocates respond to this?
A: It is clear that the Court could be leaving itself room to do additional harm to justice with this ruling. That’s because the approach that the Court adopted in Dobbs is an exceptionally narrow approach to analyze whether people have a right through the Constitution’s protection of substantive due process rights. This restrictive view is contrary to the approach taken in some of the Court’s most important decisions, including cases that protect the rights to same-sex marriage or the right to obtain contraception. This approach to judicial rulemaking could result in the erosion of other fundamental rights that Americans rely on every day. An expansive view of substantive due process, like the one taken in Lawrence and Obergefell, provides the most liberty and freedom for all Americans.
What about the concept of the “living Constitution”?
A: We share certain core values, but the way we express them changes as time passes. And that is what “living constitutionalism” is about — when we interpret the Constitution to include certain rights not explicitly enumerated in the document. The living constitution approach is also the dominant view throughout the world. Following a living constitution approach to Constitutional interpretation is not just popular, but will result in expanding rights and increasing opportunity for all Americans.
In fact, most Americans believe that the living constitution approach is the best way for the Supreme Court to analyze the Constitution[5] because it’s based on the idea that constitutional law grows and changes with the society within it. Sometimes, conservative thinkers acknowledge that it’s not, in fact, such a bad thing, and show how this is contrary to the constitutional conception of our nation. The idea of living constitutionalism allows our nation to continue to be governed by the people who live in it today, rather than the people who lived hundreds of years ago.
How do we stay energized and involved?
A: Despite this decision, the aspiration for justice and the world that we are trying to achieve must stay at the forefront. There are still many ways to protect abortion rights by advocating for legislation and executive orders at the state, local, and federal levels. We know from history as our guide that it takes time – sometimes generations – to achieve justice. And we must continue to put forward aspirational narratives that call for nothing short.
Check out other ways to make a difference here, here, and here.
Crafting Your Message
We recommend that you use VPSA when communicating about this issue. VPSA is a communications structure – Value, Problem, Solution, Action – that guides the creation of values-based messages that motivate audiences to action.
Leading with VALUES creates broad points of agreement and shared goals that will resonate with nearly any audience. Being explicit about the PROBLEM, and how it threatens shared values, creates a sense of urgency and connects individual stories to broader systems and dynamics. Offering a SOLUTION gives audiences a sense of hope and motivation. The best solutions are connected directly to the problem offered and make clear where the responsibility for change lies. Assigning an ACTION gives the audience a concrete next step that they can picture themselves doing and creates a feeling of agency.
Sample VPSA Messages
Autonomy
VALUE
We should have control over what happens in our own lives. Autonomy means having self-directing freedom over our choices regardless of our race, sex, gender, or class.
PROBLEM
The Supreme Court’s Dobbs opinion is an affront to those freedoms. It prevents the autonomy of those with the ability to bear children, especially those from minority, marginalized, and low-income groups. The Court’s opinion permits states to infringe on the right to an abortion and destroys self-determination for those living in more than 25 states. Not only that, but the Dobbs opinion also jeopardizes other basic rights such as interracial marriage and same-sex marriage.
SOLUTION
The journey to reaching justice must continue. We have the power to encourage federal and state representatives to act, to influence public opinion and, in turn, to influence the outcome of future elections and the future makeup of the Supreme Court. We can also provide aid to organizations helping poor and marginalized communities access safe abortions.
ACTION
It is essential to use your voice and get involved to end the Court’s attack on basic human rights. Vote in every election. Talk to your friends and family about the importance of reproductive autonomy and freedom. Push your representatives for legislation and executive orders at the state, local, and federal levels.
Opportunity
VALUE
Everyone deserves equal opportunity. We must work to break down barriers that prevent equal opportunity based on race, sex, gender, and class.
PROBLEM
The Dobbs opinion destroys opportunity for those who can bear children and will hit members of the Black and brown communities hard. Dobbs astronomically increases the financial burden of obtaining an abortion. Low-income people, many of whom are Black and brown women, Black and brown transgender men, and Black and brown non-binary persons, will suffer the brunt of that blow.
SOLUTION
In light of Dobbs, we must work to decrease the financial burden of obtaining an abortion for low-income people. States and organizations with resources should support people who now need to travel out-of-state to secure their reproductive rights.
ACTION
Governments and organizations should provide travel grants and other resources so people from states with limits on abortion rights can afford the costs of travel to obtain an abortion. Individuals with the means can support organizations that do so, and can push their elected representatives to take action.
Narrative Principles for Discussing Supreme Court Cases
As the Supreme Court prepares to issue its final decisions of the term, it is vital that we remember the values which underly the essential liberties we strive for. Although our hope is that the Court will ensure that everyone can fully enjoy the protections and rights provided by the Constitution, there are a number of cases pending that could set us back on this aspiration. This includes challenges regarding the extent to which local governments can take steps to prevent organizations from discriminating against LGBTQ couples who want to foster children; whether states can constitutionally restrict voting; and whether the healthcare protections in the Affordable Care Act remain constitutional, among other important cases.
The Opportunity Agenda strongly believes that it is important to uplift the need to protect the hard-fought gains our country has made in promoting and preserving opportunity, while also acknowledging that these hard-fought gains are, in many respects, still incomplete. It is on this premise that we prepare ourselves to critically analyze Supreme Court decisions that might undermine the very progress that has been achieved.
We encourage communicators, advocates, and anyone concerned with social justice to uplift the important point that Supreme Court justices must preserve prior decisions that protect and advance constitutional rights. Below are some suggestions for how to do this, informed by recent opinion research for talking about the Supreme Court as it gets ready to issue these end-of-term decisions.
General Advice
Focus on what Supreme Court decisions mean to our shared values. Most audiences are not at all familiar with – or even focused on – the outcomes of Supreme Court cases and their impressions will be shaped by headlines and topline rhetoric. It’s important to find ways to engage at that level. A great way to do this is to focus on values, such as reminding people of the kind of country we want to be and drawing on our best ideals. Consider what the decision suggests for the celebration or undermining of those values. Values: Justice, Freedom, Dignity, Fairness, Opportunity, Democracy, Family.
Don’t focus on what a decision is not. Discuss what it is. Explaining the legal details of what the case does not mean is less powerful than affirmatively stating what it does mean. Spending too much time “myth busting” or telling audiences that the ruling does not outlaw abortion, for instance, only repeats the phrase and strengthens it in audiences’ minds. Remember that “myth busting” doesn’t result in audiences remembering your point – it instead results in the further penetration of the points that opponents make.
Pivot to solutions and action. While reporters covering the case may want “just the facts,” there are many opportunities to remind audiences of the solutions that the case highlights, and what they can do to make those solutions happen. Progressive and base audiences will be fired up to do something to celebrate or express anger or discontent, so make sure to provide a concrete action. Sympathetic audiences need to be primed to feel as though their efforts matter, and that they can be both despairing of this moment in history, while at the same time remembering that our country’s core principles and history are to slowly make progress even through challenging times. Undecided audiences need to hear the positive alternatives that are possible. Values: Pragmatism, Common Sense, Innovation, Determination to Do the Right Thing, Our Shared Responsibility to Fix Flawed Policies, Solidarity.
Specific Advice for the Pending Decisions
1. LGTBQ Justice and So-Called Religious Freedom
Fulton v. City of Philadelphia
The Supreme Court will be deciding whether the City of Philadelphia improperly terminated its relationship with a Catholic charity that refused to screen same-sex couples as foster parents. The City of Philadelphia refused to work with this charity because of its discriminatory screening practices. Now, the charity is arguing that this termination violated its right to freedom of religion. This case presents a conflict of rights in which the City of Philadelphia is concerned with same-sex couples’ right to be free from discrimination, and the charity is claiming that it has a right to religious freedom in its discriminatory decision not to work with same-sex couples.
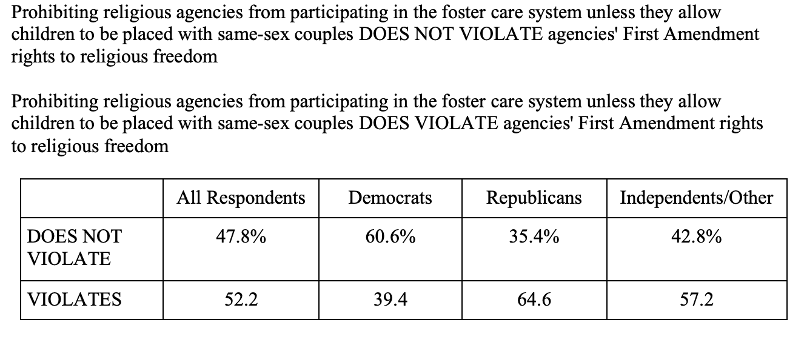
Recent public opinion research is helpful in assessing how to respond to this case and the others that are before the Court this term. A recent study polled a nationally representative sample of 2,158 American adults about their views on upcoming Supreme Court decisions[1] The SCOTUS Study asked respondents whether they believed that requiring foster agencies to place children with same-sex couples violated the foster agencies’ right to religious freedom, and 52.2% of the public stated that it does violate these agencies’ right to religious freedom.
This finding suggests communicators and advocates should emphasize the government’s role in preventing discrimination and in ensuring that everyone is able to build a family with dignity. Emphasizing the government’s role in preventing discrimination and the importance of protecting everyone’s right to family and equal justice – including the rights of potential LGBTQ foster couples and their prospective foster children – will be critical. Moreover, communicators and social justice leaders should connect the outcome in the case to our shared values by describing how the outcome in this case might undermine or bolster local governments’ abilities to prevent discrimination.
Values to Uplift When Discussing This Case: Family, Equal Justice, Human Rights, Community, Empathy.
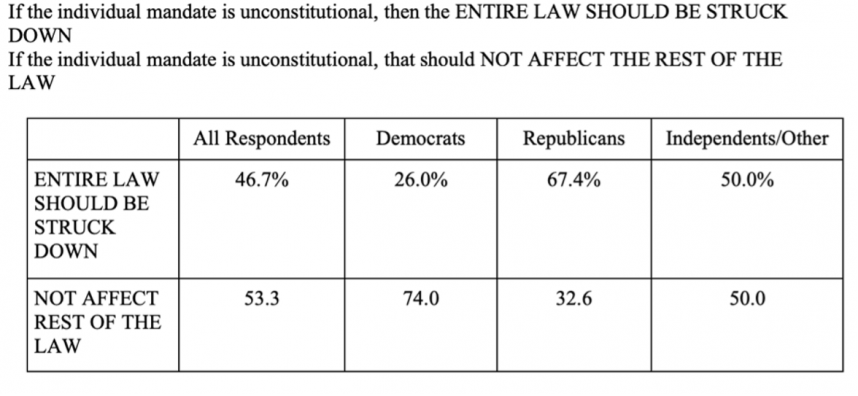
2. Affordable Care Act
California v. Texas
Following its 2012 decision upholding the Affordable Care Act, the Supreme Court will again be deciding upon a challenge to its constitutionality. The Court will decide on two main issues: (1) whether the individual mandate is constitutional; and (2) if the individual mandate is unconstitutional, whether it is nevertheless severable from the Affordable Care Act, allowing this Act to remain in force even if the individual mandate provision is no longer part of it. While it is possible that the Court will not decide upon the substance of the case and will instead find the parties who brought the case to not have standing, it is important to plan for the decision, nonetheless.
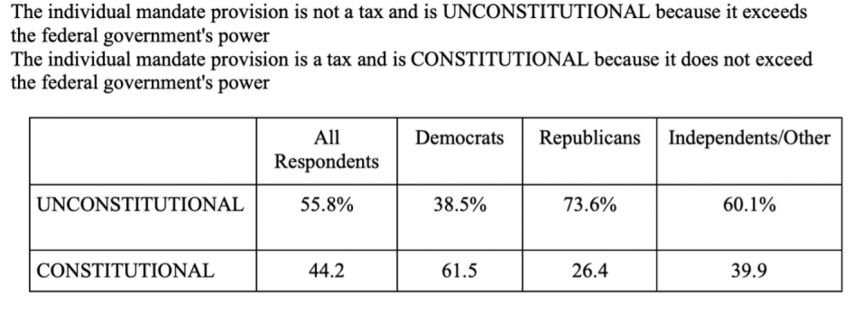
The SCOTUS Study found that 55.8% of respondents believed that the individual mandate is unconstitutional. This finding suggests that there is additional work needed to explain how the mandate broadens access to healthcare and is critical to a better-functioning healthcare system.
If the Court strikes down the mandate and thereby strikes down Obamacare, it will be important to emphasize how the Supreme Court’s choice was excessive and that millions of Americans will be left uninsured by it.
Remind audiences of our responsibilities to our fellow human beings. Access to healthcare is incredibly important and should be uplifted as a value, and after enduring the COVID-19 pandemic, audiences may be more open to these messages than ever before. As we are starting to see glimmers of hope regarding the progression of the COVID-19 pandemic, it remains important to protect everyone’s access to healthcare.
Values to Uplift When Discussing This Case: Human Rights, Community, Health, Empathy, Compassion, Looking Out for One Another.
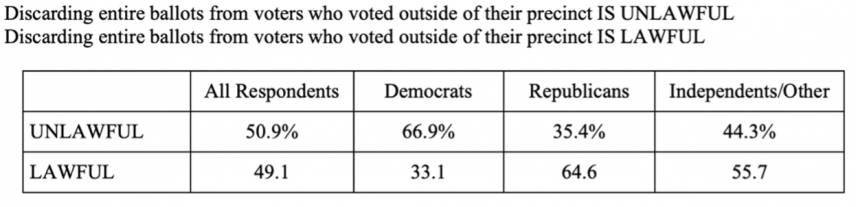
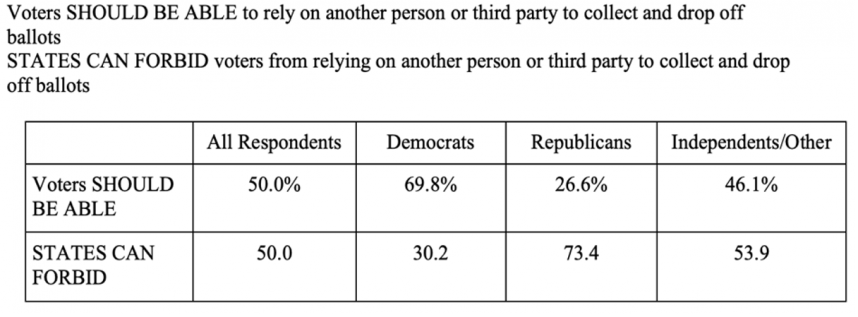
3. Voting Rights
Brnovich v. Democratic National Committee I
Following Donald Trump’s false claims about the 2020 election, his followers have initiated a massive effort to both continue the drumbeat promoting fraud and suppress voter turnout in many states. For example, Arizona passed a law that (1) prohibits people from getting assistance from others to drop off their ballots on their behalf, and (2) requires that provisional ballots be automatically discarded when a voter votes in the wrong precinct. According to the SCOTUS Study, voters are evenly split on how the Court should resolve these two issues.
The widespread, “big lies” about the 2020 election present unprecedented challenges to our democracy and warrant bold action. The response to the Supreme Court’s decision in this case should emphasize the Court’s role in ensuring that every citizen is able to exercise their right to vote. The Court’s decision may include a ruling about the appropriate standard for challenging voter suppression efforts, which may or may not make it more difficult to contest these threats to our democracy.
Values to Uplift When Discussing This Case: Democracy, Equal Justice, Human Rights, Community, Fairness.
4. Criminal Justice
Terry v. United States
Taharick Terry was convicted for possessing just 4 grams of crack cocaine, the equivalent weight of around four paper clips. He was sentenced to more than 15 years in prison because of a law that produced a 100:1 sentencing disparity for crack cocaine as compared to powder cocaine. This disparity contributed to gross racial inequities in sentencing by targeting the form of cocaine – crack cocaine – that is more prevalent in Black and brown, and lower-income, communities for grossly higher sentences than its powder form.
In 2010, President Obama and Congress reduced the disparity to 18:1 in the Fair Sentencing Act. In 2018, Congress passed the First Step Act, which allowed sentencing reforms to apply retroactively to people already sentenced in prison because of draconian sentencing laws. This case addresses whether offenses like Terry’s fit within the provisions that allow for less serious offenses to be re-sentenced. The decision in this case could have a broad impact on efforts to address some of the harms of excessive and racially biased sentencing laws.
Values to Uplift When Discussing This Case: Equal Justice, Fairness, Human Rights, Community, Family, Due Process.
Conclusion
As a general matter, it is important to communicate carefully, as the first read of any decision can sometimes mislead communicators into saying something they come to later regret, or to say something that isn’t quite the message that is important to uplift. It is therefore especially important to carefully review the Court’s holding(s) in each case and consult those who are working directly on interpreting and commenting about them. Sometimes it may be beneficial to narrowly construct any comments on a decision when formulating your response. Don’t comment until you’ve seen the facts and the lead party’s statement, as well as consulted with those most closely connected to the story that social justice leaders are recommending. Remember, the first statement you make will be the most powerful. Regardless of the outcome, it is beneficial to emphasize how values represent our vision for the aspirations we have for our country, and the importance of what the Supreme Court means to those values.
[1] Stephen Jessee, Neil Malhotra, & Maya Sen, “What Do The American People Think About the 2021 Supreme Court Cases? Results from SCOTUSPoll, a collaboration between researchers at the Harvard Kennedy School of Government, the Stanford Graduate School of Business, and the University of Texas” (April 22, 2021), https://projects.iq.harvard.edu/files/scotus-poll/files/scotuspoll-summary2021.pdf.
As we process, discuss, and continue to respond to the January 6th attack on our democracy and what it means for the days leading up to the Inauguration and beyond, The Opportunity Agenda offers a few messaging ideas for the immediate moment that also advance a long-term vision for justice.
Together, we must put forth a strong and unified message that names the hypocrisy and violence that white supremacists perpetuated at our nation’s Capitol on Jan. 6. We must call for those who inspired and carried out this insurrection to be held to account, and we must uplift the aspirations and vision we are striving for our democracy to be. Our communities and our country’s ideals depend on it.
1. Lay out a long-term vision, framed with values. In crafting your message, uplift the values that serve us in the current moment while also strengthening our long-term narrative. For instance:
Voice: Our Democracy depends on ensuring that all our voices are heard, and votes counted. The history made in Georgia in the runoff election on Jan. 5, with BIPOC organizers and voters leading the way with their organizing prowess, voices, and votes, cannot be overstated, and we must continue to celebrate this #BlackJoy and #JoyToThePolls as progress for our democracy – it is a defining moment for what our country aspires to be. The values of Voice, Community, and Inclusion ruled the day in Georgia and in the nation with record voter turnout – particularly Black, Latinx and APIA voters — and with the historic election of Rev. Warnock to the U.S. Senate. It is progress that we should continue to celebrate and uplift loudly despite everything else we are witnessing and facing.
Safety: We must ensure the true safety of everyone, whether they are working a job during the pandemic, peacefully protesting, or experiencing an encounter with law enforcement. We can use the jarring memory of the January 6th actions at the U.S. Capitol as a stark reminder that we must commit to doing all that is in our power to promote true Safety for all. This means resoundingly rejecting white supremacy’s grasp on our society, our police departments, the White House, and all who enable it. We will not stand for a system that is complicit with the violence promulgated against Black protesters, while at the same time is easy going on white vigilantes who run roughshod on federal spaces.
Dignity: Because we are humans first, and all people deserve to live in peace and dignity. We must remind people that our new future is built upon everyone having a voice, all of us coming together as a community to solve shared problems, keeping each other safe, and helping each other live with Dignity. We cannot go back to business as usual because that is what led to this crisis. We must take bold action to make this country a true, inclusive democracy where we stand with and for each other and where our elected officials and public servants respect our rights, no matter who we are.
2. Emphasize moving forward. Many of the events of the past year have reminded us of some of the country’s worst instincts and darkest history. But we have a moment now to underscore with audiences the message that we can move toward a better version of this nation if we come together to address our shared challenges and go beyond. Emphasize your long-term vision and paint a vivid picture of that future as well as the clear actions we need to take to achieve it. Remind people that to move forward, we have to come together in our diverse experiences, ideas, and strengths to build an economy, society, and country that truly embraces and embodies justice and opportunity. This means fighting for transformational changes, not accepting incremental or piecemeal solutions that leave people out and put us on a sluggish path toward our vision. We have a moment, and we must seize it.
3. Build messages that move your long-term narrative. The events at the Capitol and the actions of this administration, both recent and over the past four years, represent much of what is wrong with our country. But remember to choose your examples carefully to build your story for moving forward. For instance, the hypocrisy of law enforcement’s response to the white nationalist attack on the Capitol compared to their stealthy and violent strong handling of Black Lives Matter protesters over the summer makes a powerful argument for those who are advocating to Defund the Police in favor of building community resources for achieving true safety. Also, those focusing on Democracy work may choose to highlight the president’s attacks on voice and vote that culminated in January 6th’s violence. Spending too much time describing or explaining all the many dimensions of a specific event will likely keep audiences in that experience rather than looking forward – so remember to keep a simple framework for talking about the Values, Problems, Solutions and Actions we are trying to share.
Our nation can and should be a place where everyone enjoys full and equal opportunity. We are strongest when we all have a fair chance to achieve our full potential, contributing fully to our economic engine and social fabric. When everyone has the tools to support themselves and their families, the benefits flow to individuals, communities, and our nation as a whole.
Key to that full and fair opportunity is the ability to pursue gainful work while maintaining a safe and healthy life for one’s children and family. Yet, in our changing economy, that opportunity is increasingly at risk as Americans must make the unacceptable choice between caring for sick family members and earning the full salary needed to support that family. Access to paid family and medical leave determines whether parents can care for a new baby or sick child, whether a dedicated worker can also dedicate time to an ailing or dying elderly parent, and whether a family health emergency will also become an economic catastrophe. Despite significant public support, political will has been lacking, leaving working families and national economic opportunity at risk. According to the National Compensation Study, only 14% of civilian workers had access to paid leave in 2016. Federal law has remained stagnant on the issue since the Family and Medical Leave Act (FMLA), which requires unpaid leave, passed in 1993, and state and local progress has been slow and uneven. The lack of paid family and medical leave burdens families of all backgrounds. It also worsens patterns of unequal opportunity based on race, ethnicity, gender, and income.
On behalf of the Opportunity Agenda, Lake Research Partners (LRP) conducted a review of research studies related to paid family and medical leave. This literature review synthesizes and summarizes relevant opinion research findings about attitudes toward paid family and medical leave. This report provides a detailed overview of gaps in existing internal and external public opinion research alongside a summary of what messages, messengers, mediums, and platforms have been most effective to date.
Findings
Current Paid Family and Medical Leave Legislation
States are leading the way in implementing legislation to provide paid caregiving, parental, and medical leave.
On the national level, both Democratic and Republican legislators want federal paid family and medical leave legislation but disagree over what to cover and how to fund it.
Democratic voters tend to be more supportive of paid family and medical leave than Republican voters. However, there is a gender gap among Republicans.
Attitudes on Paid Family and Medical Leave: Small Business Community
Small business owners are supportive of paid family and medical leave, which could give them a competitive advantage, but many would prefer that employers be allowed to choose whether to provide paid family and medical leave.
Polls show that there is a great deal of support for paid family and medical leave in the United States and the support is bipartisan.
In addition to supporting a national paid leave policy, most Americans are also willing to contribute to funding for such a program.
Insights from dyads and focus groups conducted by Lake Research Partners suggest there may be opportunities to build support for paid family and medical leave among women of color and Independent/weak Republican women.
Working families respond best to messaging around paid family and medical leave that talks about helping your family and being there for them and that addresses the caregiving needs a person may have beyond simply parental leave.
Attitudes on Paid Family and Medical Leave: Caregivers
As the elderly population continues to grow, so does the number of people who are involved in informal caregiving of older family members. According to the Bureau of Labor Statistics, 16% of the employed civilian population provided unpaid care to someone with an aging-related condition.
A growing number of Americans are recognizing the need to provide paid leave to care for an elderly family member who is seriously ill, injured, or disabled.
Access to paid family leave has demonstrable economic impacts, and lack of access has consequences.
Attitudes on Paid Family and Medical Leave: Communities of Color & Non-Traditional Families
A disproportionate number of those in communities of color do not have access to paid leave. A national paid leave policy would ensure equal access to paid leave.
FMLA does not recognize same-sex relationships, so employers are not required to provide leave to care for a same-sex partner or spouse. Access to paid leave is a major concern for LGBTQ workers.
Effective Messaging for Paid Family and Medical Leave
Determining the best messaging and language that will move voters from support to action on a national paid family and medical leave policy is critical as both Democrats and Republicans prepare for the 2020 election cycle.
Voters respond well to several of our key values in messaging, including the importance of family, the freedom to do what is right, and the recognition that caregiving is part of life.
Statements that focus on the positive impact of paid leave on economic security and not having to choose between giving care and getting a paycheck have a powerful and positive effect on voters and activists. Word choices like “workplace” or “public” do not affect results much.
The words used in a message, especially the first few words or “kickoff phrase,” can increase or decrease support. It is important to know how different audiences respond to particular words and statements.
Our research report, Power of Pop: The Case of the Cultural Influencers, underscores the potential of celebrity not only to spotlight social issues, but also to spark meaningful dialogue and action that can lead to lasting policy and social change. These tips are intended for those who work with cultural influencers of all kinds – not only luminaries in entertainment and sports, but also the wide range of influencers who are in a position to harness the energy of fandom and media to inspire large audiences and help shift cultural norms. We hope these tips help you increase your impact for social change.
1. Seek out guidance from frontline advocates.The people most directly impacted by an issue can provide essential expertise to make an influencer’s efforts meaningful. Find groups that are led by or deeply embedded with frontline communities and listen to their policy priorities and proposed solutions. What are their goals and how do they want people to feel, think, and talk about the issue?
2. Determine the influencer’s unique role.To determine where an influencer could add the most value, look for the intersection of: 1) the cultural and political changes needed to get to the desired solutions, and 2) the ways in which the influencer can contribute given their interests, skill sets, and platforms. For instance, if the debate around an issue is being dominated by destructive perspectives, how could they help reframe the conversation? If an issue is not gaining broad attention, how could they put it in the spotlight? If an issue is in the public eye but not broadly supported, how could they create the cultural symbols or stories that will help define the issue and build its popularity?
3. Choose the influencer’s tone and approach.If an influencer is a public figure, then what they say or do in public impacts their brand. It is useful to carefully consider what about their brand could make them especially effective. If an influencer is known for playing a universally loved character in films, they might be in a position to help bridge political divides. If an influencer is known for a character (or previous personal statements) that identifies them as having a particular worldview, they might be in a position to
mobilize supporters to take action. Decide in advance what kind of tone and approach would align with an influencer’s existing brand or would intentionally expand that brand in directions the influencer would want. Remember that maintaining influence with an audience is usually dependent on choosing a tone and approach that is congruent to this brand.
4. Identify your target audience and where to reach them.Different platforms have the potential to reach different audiences. It is important to be clear on your goals in order to determine which audiences an influencer might aim to target. For example, if an influencer’s goal is to raise awareness about the impact of mass incarceration, and their fan base is made up primarily of communities who have already been deeply impacted by that issue, then they might look at engaging platforms that could reach beyond their fan base, (i.e., social media or events hosted by other influencers). If the goal is to reframe how people think about an issue familiar to their audience, such as rethinking bail reform, then engaging platforms that target their fan base, (i.e., fan sites or social media channels) would be the more effective strategy
5. Establish shared values.Research shows that audiences are more receptive to unfamiliar arguments when they are framed with shared values. Values are our most fundamental principles and they become a means of establishing a human connection that can cut through stereotypes and partisan suspicion. Facts and figures can be tuned out or disregarded, but values activate emotions, invite common ground, and open minds to new ideas. Influencers should identify the values that motivate them, and lead with those values when talking about the issues. It would also be worthwhile to explore how an influencer might use their creative skills and platforms to encourage or model those values.
6. Plan ahead how you will center frontline voices.It can be tempting for the media and public attention to focus on an influencer’s actions rather than the issues they are trying to raise. It is important to take extra steps to incorporate the voices and perspectives of those traditionally overlooked or excluded from public discourse and ensure that credit is given to grassroots activists and/or community organizers who are already leading the charge in social change efforts. Partnering with frontline groups – which requires building relationships and trust – can be very helpful in deciding whose voices and/or which stories should be centered.
7. Find allies.For most social and political change efforts, there is power in numbers. Find like-minded influencers who would be willing to join in a coordinated effort, or at least amplify when the influencer decides to speak out or take action on an issue. Find organizations and activists who would be willing to coordinate with and/or publicly support the influencer. Lining up these allies can be especially important, not only to increase the impact of the message, but also to help protect the influencer from becoming a target for industry or public reprisals.
8. Link the influencer’s personal story to the larger story.Authenticity matters. Our research shows that news coverage favors individual storytelling by directly-impacted influencers. If an influencer isn’t directly impacted, they should find ways to share what about their own experience compels them to support an issue. Additionally, personal stories should link to systemic issues. In telling the story of one child’s family who isn’t able to pay for a needed surgery, an audience might become motivated to provide an individual solution, solving only that one family’s problem. But to motivate an audience around a systemic solution, (i.e., universal healthcare), an influencer should link that child’s story to the larger issue: the fact that millions of children do not have healthcare coverage.
9. Write a mission or artist statement.An initial written or artistic statement laying out an influencer’s reasons for speaking out will likely become a foundation for future discussion. If an influencer takes subsequent actions, the media will likely continue to quote the original statement, which will help frame the debate as long as the influencer garners public attention for the issue. When drafting a statement, feedback should be sought from various sources, with priority placed on incorporating the feedback of those directly impacted: individuals and communities regularly excluded from national discourse. Our “Establish Shared Values” tip above may provide valuable guidance for drafting a statement.
10. Make use of replicable symbols or imagery.The power of symbolism and imagery has emerged as a key cultural tool to keep issues in the public eye and motivate supporters to take action. Symbols and easily replicable content create avenues and inspiration for widespread participation. Think about how many athletes have now taken a knee to uplift racial justice, or how many people are now using the “Wakanda Forever” salute. A symbol can boil down a complex idea into something that is replicable, digestible, and accessible. When an influencer is planning what action to take, consider how they can integrate an element that supporters can replicate. It is important to take extra steps to incorporate the voices and perspectives of those traditionally overlooked or excluded from public discourse.
In recent years, the power of popular entertainment to inspire large audiences and shift cultural norms has become a topic of growing interest in the social advocacy space. A large body of research has been dedicated to tracking representation trends in film and television, and a growing cohort of organizations provides practical recommendations for those seeking to leverage popular culture in their advocacy work. While existing research has provided critical insights into the effectiveness of high-profile spokespeople in short-term campaigns and fundraising, significant gaps in the literature exist in terms of in-depth analysis of more symbolic actions on the part of high-profile individuals as well as measurements of the impact of celebrity influencers on long-term narrative shift.
Under which circumstances do cultural influencers have the greatest ability to achieve their goals?
Currently there is a pressing need to better understand the potential of high-profile influencers to not only draw attention to social issues but also spark meaningful dialogue and actions that lead to lasting social and policy change. As part of our Power of Pop series, this current research examines three cases of high-profile entertainers and athletes speaking out or advocating for a social and/or policy change. The cases include: Case 1: Colin Kaepernick and the Take A Knee protest Case 2: Jimmy Kimmel and the healthcare debate Case 3: Me Too and Time’s Up movement This research aims to better understand the unique influence of high-profile athletes and entertainers and provide practical recommendations for those seeking to work directly or indirectly with cultural influencers to shift narratives and effect policy change. Key questions explored in the research include:
Under which circumstances do cultural influencers have the greatest ability to achieve their goals?
Are cultural influencers’ interventions best suited for long-term cultural change, short term policy shifts, or other types of impact?
What types of celebrity intervention have the most impact?
How can social justice advocates best support/leverage the influence of cultural influencers both through direct and indirect contact?
To evaluate the effectiveness of the range of strategies and issues covered in our selected case studies, we established the following criteria for success:
If the action or sets of actions had a clearly stated goal, to what extent was this goal achieved?
Was there a marked impact on the national discourse, in both media coverage and public discussions of the issue the cultural influencer was addressing?
Did the actions of one influencer encourage others to speak out or also act?
Were there unanticipated shifts in the public discourse (and, where applicable, policy change) as a direct or indirect result of a cultural influencer’s actions?
Based on these criteria, we conducted a media content analysis and social media analysis for each individual case. Our findings point to a series of lessons learned and best practices for future cultural campaigns.
The Impact
Taken together, our findings demonstrate that strategic engagement from high-profile influencers can have the following impact on social advocacy campaigns:
Significant increases in news media and social media engagement with social justice issues: All three case studies revealed a marked increase in both the volume and focus on news media and social media engagement. For instance, since Colin Kaepernick and other athletes began taking a knee, news media coverage of police misconduct has nearly doubled (from an average of 4000 articles to 7000 articles published every 12 months), and social media engagement with the issue has seen a nearly three-fold increase.
Direct or indirect policy and cultural changes in organizations and institutions: The case studies in this report have resulted in a myriad of organizational policy and cultural shifts as a direct and indirect result of the efforts of high-profile influencers. In the case of Jimmy Kimmel, the Graham-Cassidy bill was ultimately defeated. Since Kaepernick and other athletes began taking a knee in protest to police killings of unarmed people of color, the National Football League (NFL) and several teams have spoken out in support of criminal justice reform. For instance, in September 2016, shortly after Kaepernick’s first field-side protest, the San Francisco 49ers announced that it would be donating $1 million to two charities in the Bay area focused on racial and economic justice. In January2018, the NFL in conjunction with players formed the “Let’s Listen Together” coalition, which aims to improve police and community relations. As of July 2018, 10 NFL teams have announced the launch of new committees, coalitions, or other activities aimed at raising awareness and tackling social justice issues. The Me Too movement has had a similar impact. Since the Me Too movement first began to proliferate in October 2017, more than 800 high-profile figures have been publicly accused of harassment, sexual assault, rape, workplace misconduct, and other related behavior. A recent article details the range of policy changes that have been introduced across industries because of the Me Too movement. This includes the introduction of mandatory annual anti-harassment trainings for lawmakers and staff in Congress and the inclusion of so-called “Weinstein Clauses” in several large mergers and acquisitions.
Encouraging other high-profile individuals and members of the public to speak out: Each case study was characterized by high-profile influencers successfully encouraging others to speak out in support of or opposition to an issue. Following a series of monologues from Jimmy Kimmel, several Republican senators spoke out openly against the Graham-Cassidy bill, eventually leading to its defeat. Since Kaepernick first begin his protest in August 2016, more than 200 athletes have sat or kneeled during the national anthem. Our analysis revealed that a significant portion of news media and online discourse focused on actions and commentary of other high-profile athletes and spokespeople. In the case of the Me Too movement, not only did the personal stories of high-profile entertainers propel the issue of gendered violence into the national discourse, but also subsequent coordinated efforts of the Time’s Up campaign maintained engagement with the issue after media coverage began to wane.
Why This Is a Supreme Court Nomination Like No Other, and What We Should Do About It.
When President Trump nominated Judge Brett Kavanaugh to replace retiring Supreme Court Justice Anthony Kennedy, it was clear to us that while Kennedy’s legacy is complicated, the man Trump named to replace him is not.
Based on his positions on the constitutional and legislative protections that serve all Americans, from women’s freedom to make decisions regarding when—and whether—to start a family; to the constitutionality of the Affordable Care Act; to marriage equality; to equal justice under the law irrespective of race, gender, and other aspects of who we are, Kavanaugh’s nomination would move the Court sharply and immediately away from the values we hold dear and give him the opportunity to shape court decisions that will affect generations.
Equally—if not even more—disturbing is that President Trump is seeking to name a pivotal justice to the very court that will likely rule on any criminal charges brought against him and his administration, and on the Russia investigation, which he has maligned and tried to delegitimize since the start of his presidency.
This is particularly alarming because Kavanaugh is the only one on the list of candidates who has made clear that the president of the United States is above the law. He does not believe that a president should be held accountable through an independent investigation while in office. Thus, Mr. Trump seems to have intentionally selected Brett Kavanaugh for a seat on the Supreme Court not only because of his hard-right, pro-corporate record, but also because he will not provide the very checks and balances that the framers of our Constitution intended in creating a Supreme Court.
Brett Kavanaugh’s ultra-conservative bona fides are certainly not unique, nor is it surprising that he is Trump’s pick. After all, President Trump proclaimed that he would choose a Supreme Court candidate(s) from The Federalist Society and The Heritage Foundation–prepared list, mentioned above.
But the point isn’t just that we must do all that we can to prevent the likes of the hard-right ideologue Brett Kavanaugh—and, frankly, anyone on a list recommended by The Federalist Society and The Heritage Foundation—from ascending to a seat on the high court.It’s that The Federalist Society and The Heritage Foundation created the list the president is considering in the first place, over a bipartisan set of thought partners more representative of America. And it’s especially troubling that these institutions appear to know much more about Brett Kavanaugh and the others they selected than perhaps even the senators who will eventually vote on the nominee.
At this point, we don’t know whether, or how, aspects of Kavanaugh’s record will come forward. We also don’t know, given the events of recent days, whether there are aspects of that record that are being deliberately hidden from the American people.
While it is essential to gain information about the record of any candidate to the Supreme Court, we must also do all that we can to spotlight the fact that any Trump nominee, under these circumstances, would be in the constitutionally unacceptable position of ruling on critical legal questions relating to his investigation or prosecution.
Kavanaugh’s nomination, moreover, comes at a time when Trump has repeatedly demonstrated his fidelity to the president of Russia, while at the same time denigrating the U.S. intelligence community, his own Department of Justice, and America’s closest allies. We cannot be certain that, as Supreme Court justice, Brett Kavanaugh’s loyalties would lie with the American people and the Constitution over the interests of a president who appointed him and an administration that has kowtowed to the likes of Vladimir Putin.
Our constitutional values—the separation of powers and checks and balances—could not be more important to our freedom than they are right now. The stakes for our democracy, in other words, could not be higher.
Therefore, President Trump’s ability to choose a nominee to our nation’s highest court—especially a hard-right nominee who may not hold the president accountable—is a call to action that must be answered with an even greater, more focused level of strategy, creativity, and collaboration than ever before.
We know it’s an uphill battle, but it’s one that we can win.
History reminds us that defeating Supreme Court nominations is difficult. It also reminds us of the importance of endurance. The last successful challenge to a Supreme Court nomination was the defeat of Judges Robert Bork and Douglas Ginsburg in 1987. Before that, it was Clement Haynsworth and G. Harrold Carswell in 1969 and 1970, respectively, both of whom were defeated based in part on their ties to white supremacy. In those fights, social justice leaders came together to make clear to the Senate and the American people that the nominees—and the president’s intent in nominating them—were out of sync with our national and constitutional values. The justices ultimately seated in those instances were Justice Harry A. Blackmun in 1970 and Justice Kennedy in 1987.
While today’s landscape is even more challenging with a polarized Senate, an emboldened and extremely vocal opposition, a chaotic political and media environment, and the absence of the filibuster as a tool for moderation and consensus building, we must be in it to win, and not just for the short-term, but for the long game. Let’s not forget how Kavanaugh’s supporters unjustifiably and unapologetically blocked President Obama’s nomination of moderate Judge Merrick Garland and seated Justice Neil Gorsuch. Our actions must emulate the same stick-to-itiveness that those supporters continue demonstrating today. They are running the marathon, not the sprint, and they are now even more aligned to move the Court sharply away from constitutional rights, values, and accountability.
Thus, these extraordinary times call for each of us to dig deep and offer new and innovative approaches in our work to define Brett Kavanaugh as unfit for the Supreme Court. They call for strategies that will disrupt the usual process through any lawful means necessary, using all resources and allies at our disposal. So, while Kavanaugh’s record on the issues that are at the heart of our American ideals is—and should be—dissected, we must also keep the end goal in mind and operate accordingly. This means making this fight about the foundation of our democracy—not only about one seat on the high court.
To win, we must implement the following strategies at the same time:
Join our SaveSCOTUS.org allies and others in continuing to prioritize a strategic mix of (a) persuading undecided audiences in pivotal states including WV, AK, ME, ND, and IN; (b) activating base audiences in the pivotal states and other parts of the country; and (c) delegitimizing and disrupting the opposition wherever possible. The current swing-state focus on protecting the Affordable Care Act and Roe v. Wade, although necessary, should be only one tool to move persuadables and motivate segments of the base.
Establish as a primary goal that we must convince a critical mass of political, cultural, and opinion leaders that President Trump’s actions and the open investigations into his administration should disqualify him from naming a Supreme Court justice. We must do all that we can to normalize the understanding that President Trump is a suspect in multiple cases of historic and constitutional magnitude and, therefore, cannot constitutionally or ethically be permitted to choose the justice who will likely decide his case.
Make popular culture a major force in the effort on par with other, more traditional tactics. This requires letting creatives create in their own ways, while tying their work to a common goal and overarching narrative. The 2008 Obama campaign’s flexible partnerships with artists, musicians, and cultural influencers is a recent model worth emulating and upscaling.
Step up the use of traditional and digital media to broaden the scope of bipartisan opposition to Kavanaugh. This is where traditional approaches such as op-eds, editorial board meetings, white papers, and the like will be most helpful, creating a drumbeat of voices calling for a halt to the process on constitutional grounds while making the substantive case against the nominee and his extremist supporters.
Call out the dangerous constitutional crisis into which the president has plunged our nation and make clear the solutions needed to right the ship. That, in turn, necessitates choosing messaging and content of visceral dramatic value, one example being recent audio of immigrant children in detention pleading for their parents. That intensely emotional content was the tipping point that coalesced with litigation, advocacy, and other strategies to change the narrative and some aspects of policy. It is a dynamic that we must learn from and consider utilizing.
Significantly step up criticism of the colossally inappropriate role—and extremist and un-American values—of The Federalist Society and The Heritage Foundation in selecting the judges who should rule fairly for the whole nation. As already noted by some advocates, the failed federal circuit court nomination of The Federalist Society member Ryan Bounds based on his racist writings should be revealed as the tip of the iceberg when it comes to those organizations’ ties to extremists.
In the context of constitutional values, remind relevant audiences at every turn of this president’s support for white supremacy and bigotry, from his criticism of Judge Curiel based on his heritage, to his slander of Mexican-Americans, to his praise of neo-Nazis in Charlottesville, to his ties with the racist “Alt-Right” movement. Also, kowtowing to Russia and embracing bigotry are vulnerabilities that arise again and again, and ones about which President Trump cannot disguise his predilections.
In the face of atrocious policies that pose serious threat to our Constitution and our country’s ideals of opportunity and inclusion, we must treat this fight differently. Alongside many others, The Opportunity Agenda sees the dire need to dig deep and stop Kavanaugh’s nomination. We must protect the hard-fought, historic gains our country has made in promoting and preserving opportunity.
Therefore, we are calling for preventing not only Brett Kavanaugh from taking a seat on the Supreme Court, but also President Trump from circumventing the constitutional accountability that its founders fully intended. Preserving our democracy depends on nothing short of that.
Understanding the Roots of Attitudes on Inequality Research
Opportunity is a deeply held value at the core of the American ethos. The belief that our nation can and should be a place where everyone has a fair chance to achieve his or her full potential is widely shared. But many believe the ideal of opportunity is in jeopardy and are willing to take steps to defend it.
In 2014, The Opportunity Agenda commissioned a groundbreaking nationwide survey to examine what the U.S. public thinks about opportunity in America and to measure public support for policies that expand opportunity across a range of issues, including jobs, education, criminal justice reform, immigration, and housing. Additionally, the research sought to gain a deeper understanding of the multiple factors that influence attitudes on inequality, contribute to an individual’s worldview, and predict people’s willingness to take action on issues they care about. Together, the survey’s findings offer critical insights for social justice leaders and organizations seeking to move hearts, minds, and policy.
To the New York State Departments of Health and Insurance:
The Opportunity Agenda would like to thank Governor Eliot Spitzer, Commissioner of Health Richard Daines, and Superintendent of Insurance Eric Dinallo for the chance to contribute to the development of a comprehensive and equitable health care system in New York. Please find included written testimony and recommendations, submitted on behalf of The Opportunity Agenda, for your New York City public hearing today, “Increasing Access to Health Insurance Coverage and Moving Toward Universal Healthcare Coverage.”
If you have any questions or would like further information, please use the following contact information:
Kevin Shawn Hsu
Associate Counsel
568 Broadway, Suite 302
New York, NY 10012
212.334.4267
khsu@opportunityagenda.org
Thank you for your consideration of this testimony.
Sincerely,
Kevin Hsu
Associate Counsel
Recommendations for Ensuring Equitable Access and Quality in New York State Health Care System Reform
Submitted to the New York State Departments of Health and Insurance by The Opportunity Agenda
October 30, 2007
The Opportunity Agenda welcomes the chance to provide testimony to the Departments of Health and Insurance to assist in the development of a health care system that provides equal access to high-quality care for all New Yorkers.
This testimony seeks to provide New York with equity benchmarks, elements of state-level health care policies and proposals that promote equitable health care access and quality for all populations, that should be used in evaluating any health care system reform proposals. The benchmarks address six aspects of the health care system: (1) Access to Health Care, (2) Quality of Care, (3) Patient Empowerment, (4) Health Care Infrastructure, (5) Policy Infrastructure, (6) Social and Community Determinants of Health. These benchmarks are informed by our review of literature on health care disparities and draw from existing and proposed state-level policies that promote equitable, high-quality health care for all.
Summary of Recommendations
In crafting a universal health care system that provides access to quality care for all residents of New York, the State should include reforms that ensure improvements to the system for all while eliminating health care disparities based on race, ethnicity, primary language and income. New York should utilize the equity benchmarks described in this testimony to evaluate any health care system reform proposal. In making health care affordable and accessible to all, including underserved communities, a health care system must ensure that cost-sharing policies are equitable by, for example, preventing policies such as premium pricing based on existing health status or individual mandates from disproportionately excluding communities of color from care. Reforms must also improve the cultural and linguistic competency of both providers and health care systems to encourage effective use of health care resources and delivery of appropriate care. In all of these efforts, New York must also integrate monitoring efforts into reforms to guarantee that changes lessen, rather than exacerbate health care disparities.
New York must also improve the quality of care that patient receive, regardless of the insurance program in which they are enrolled. With regards to eliminating the documented inequities in the quality of health care received by communities of color, immigrant communities, and low- income populations in New York, reforms must include collection of quality of care data, stratified by race, ethnicity, primary language and other characteristics of underserved communities. This data should be publicly reported and, more importantly, acted upon by providing incentives to providers who engage in quality improvement programs targeting demonstrated health care disparities, educating patients, and supporting and expanding community health worker programs that bridge cultural and trust gaps between providers and underserved communities.
Finally, New York must reform the health care system infrastructure to better address the needs of racial, ethnic, and language minorities. This includes increasing state support for and reducing the financial vulnerability of “safety net” hospitals, community health centers, and health care institutions serving poor and minority communities. Reforms should also construct or revive programs that combat disparities, such as creating incentives for health care professionals working in underserved communities, reviving the statewide network of Health Systems Agencies that used community health planning to better align community needs and health care resources, and reviewing the use of the Certificate of Need process so that changes to hospital services are contingent on community need and reduction of racial, ethnic, and linguistic health disparities. To implement these infrastructure and policy reforms, New York should dedicate resources to coordinating the various responsible state agencies in creating a comprehensive, statewide approach to eliminating racial and ethnic health disparities.
Legal and Ethical Principles
Our review of New York’s constitutional, statutory and other legal obligations, as well as public opinion, indicate that efforts to reform New York’s health care system must be informed by the following principles:
That the New York State Constitution obligates the State to provide access to high quality health care to all New York residents, with particular attention to vulnerable groups and those least able to pay for care.1
That federal civil rights laws and international human rights laws obligate the State, its subdivisions, and virtually all health care providers to avoid and actively dismantle any practices having a discriminatory purport or effect on particular racial, ethnic, or linguistic groups, with respect to access to or quality of health care.2
That federal and state health care laws obligate the State to ensure adequate support and care for low-income and medically underserved communities, including through adequate Medicaid reimbursement rates and equal treatment, irrespective of income or insurance status.3
That the people of New York overwhelmingly believe that everyone in New York has a right to health care, and that the State is responsible for ensuring that racial or ethnic minorities and low-income New Yorkers have an equal chance to access health care as do wealthy people.4
That protecting and promoting the health of the inhabitants of New York5 requires systems, policies, and practices that ensure equitable access to high quality care.6
Health Care Equity in New York
The efforts of Governor Eliot Spitzer, the Department of Health, and the Department of Insurance to move New York toward universal health coverage are to be lauded. Rapidly escalating health care costs, a rising number of people who lack health insurance, inconsistent health care quality, and a paucity of federal action to address these problems necessitates the consideration of state-level health care reform proposals that, if enacted, would create significant changes in how the State approaches health insurance coverage and health system regulation.7 A poll conducted by The Opportunity Agenda and designed by researchers at the Harvard School of Public Health confirms public support for these efforts: 89% surveyed said that “everyone in New York has a right to health care.”8
The New York State Departments of Health and Insurance are holding these hearings with the explicit goals of achieving universal, high-quality health insurance coverage and containing health care costs. However, a major problem which impacts both cost and quality, yet is often unaddressed, is the problem of inequality in health care access and quality. Inequality is a pervasive and persistent problem that is acknowledged by health care quality and policy experts to be a central concern in any heath care reform effort.9 We use the term health care inequality to describe disparate or disproportionate health care access and quality problems experienced by racial and ethnic minorities, the uninsured, immigrants, those who are not proficient in English, and others, relative to more advantaged groups. While having health insurance is the single most significant factor determining the timeliness and quality of health care that patients receive, inequality persists even among similarly insured patients. For example, a large body of research demonstrates that even with the same health problems and the same sources of health insurance, racial and ethnic minority patients, as well as those who are not proficient in English, tend to receive a lower quality of health care.10
Health care disparities are intimately linked to access, quality, and cost issues within the health care system. For example, a relatively small investment targeted toward communities experiencing significant gaps in care can save the State significant amounts of money. Consider the neighborhood of Rockaway, Queens, where 13.5% of mothers receive late or no prenatal care; unsurprisingly, a full 10% of babies in that community are born low-weight.11 While the average cost of medical and follow-up care for a healthy normal weight baby is $6,500, care for a premature or low birth-weight baby costs between $90,000 and $180,000. However, a $180,000 health promotion program will provide more than 50 at-risk pregnant women with intervention to reduce their risk of bearing low birth-weight babies; if the program is even modestly successful, it would dramatically improve the financial efficiency, as well as the quality, of the neighborhood’s health care system.12 New York State could save hundreds of millions of dollars if it ensured access to quality primary care for all New Yorkers.13 True high- quality, universal care requires recognition and efforts to eliminate the significant health care inequities facing residents of New York.
Racial and ethnic minority and language-minority groups face well-documented problems in both accessing health care and receiving equal quality care. Lack of health insurance is a primary cause of these disparities; over half of the nation’s 47 million uninsured individuals are people of color.14 In New York City, 30% of New Yorkers of color are uninsured, compared to under 17% of white New Yorkers.15 And in New York State, Asian residents are more than twice as likely to be uninsured, and Hispanic residents are more than three times likely to be uninsured as non-Hispanic Whites (Figure 1).
Figure 1: Uninsured Rate in New York State, Adults 18-64 By Race, 2007
Source: New York State Department of Health, New York State Minority Health Surveillance Report, Sept. 2007; “All races” comes from the Current Population Survey Annual Social and Economic Supplement, available from the Current Population Survey Table Creator at http://www.census.gov/hhes/www/hlthins/data_access.html.
Closing racial and ethnic gaps in insurance coverage while increasing overall insurance rates is crucial. But health insurance coverage expansions alone do not ensure that medically- underserved, predominantly-minority communities will receive quality care in a timely fashion, or that inequality in health care access and quality will be eliminated. Predominantly minority communities also face higher rates of health problems, but have fewer health care resources, such as hospitals, primary care providers, outpatient clinics, and nursing home facilities.16 The health care services that are available to them are often of lower quality than those in more advantaged communities.17 And even among minorities who have insurance, many face cultural and/or linguistic barriers to accessing care, despite the existence of federal standards for cultural and linguistic competence in health care settings.18
As described below, in addition to providing truly universal health insurance coverage, steps toward ending inequality can include collecting data and monitoring for inequality, improving the health care infrastructure in low-income communities and communities of color, and addressing these groups’ cultural and linguistic needs.
I. Access to Health Care
New York can expand access for underserved populations by:
Making health care affordable
Seeing that health care is affordable for all communities necessitates that policies take into account and attempt to minimize the disproportionate impact that health care costs may have on access and utilization among underserved populations. In creating a cost-effective and sustainable economic model for a health care system, New York should be sensitive to the potential effect of proposals on health insurance coverage and access among communities of color. Specifically, New York should:
Examine the equity of health insurance premium pricing. For example, charging people in poor health more for insurance than those in good health is inequitable, and disproportionately burdens communities of color.
Consider the equity of cost-sharing arrangements. Cost-sharing arrangements are intended to make costs more transparent and promote cost-conscious consumer behavior, but may thwart universal coverage and exacerbate disparities. Several studies demonstrate that minority and low-income communities are less likely to access health care as out-of-pocket costs rise.19
Enable those with low incomes to purchase health insurance through sliding fee scales for premiums, public subsidies, and limits on co-payments and other out-of-pocket costs such that those at the lowest income levels will face only nominal charges.
After implementing any cost-sharing policies, study and respond to potential unintended effects of cost-sharing on utilization by currently uninsured and underinsured groups.
Assessing the differential impact of individual mandates on communities of color, immigrants, and low-income populations
Massachusetts’ new statute to achieve universal coverage requires individuals and families to purchase health insurance, and also establishes standards of affordability to determine premium or cost-sharing contributions. The impact of a similar individual mandate and definitions of affordability here in New York may vary across racial and ethnic groups, even at the same income level, as these groups vary in wealth and access to resources.20 In addition, the challenges of enforcing an individual insurance mandate across different communities are significant. Some documented immigrants, for example, may be reluctant to apply for public health insurance programs, even if eligible, as a result of anti-immigrant rhetoric and policies, and might therefore be slower to comply with a mandate.21 If New York chooses to apply an individual mandate, it should monitor insurance take-up among previously uninsured people by race, ethnicity and immigration status, and take steps to correct policies that might have a disproportionate impact.
Promoting cultural and linguistic competence in health care settings
Health care providers and systems must be culturally and linguistically competent to improve health care access and quality for an increasingly diverse U.S. population.22 The federal Culturally and Linguistically Appropriate Services (CLAS) standards identify fourteen benchmarks that have been widely accepted and increasingly adopted by health systems and providers.23 Indeed, federally-funded health care organizations are mandated to meet four of the standards.24 Similarly, greater diversity among health care professionals is associated with greater access to and satisfaction with care among patients of color.25 New York must develop or expand diversity efforts, which improve the cultural competence of health systems and increase the likelihood that patients of color will access and be satisfied with the health care they receive. Specifically, New York may:
Promote cultural and linguistic competence through policies that encourage and reward health care organizations that implement the CLAS standards, such as fully reimbursing providers for language services through the Medicaid and Child Health Plus programs, or increasing payments through these programs for providers complying with the full set of standards.
Promote greater diversity among health care professionals by developing or expanding tuition-for-service agreements with underrepresented health care professionals.
Requiring cultural competency training for health care professional licensure
New York State is one of the most diverse states in the country, and New York City’s population is predominantly people of color. Demographic changes require that the health professions keep pace by training future and current providers to manage diversity in their practice.26 Some states have taken action to address this need—as of 2005, New Jersey required that all physicians practicing in the state must attain minimal cultural competency training as a condition of licensure. New York should assess whether and how various health care expansion proposals should follow suit.
Reducing “fragmentation” of the health insurance market
A potentially significant source of racial and ethnic health care disparities among privately insured populations lies in the fact that minorities who have insurance are likely to be disproportionately enrolled in “lower-tier” health insurance plans. Such plans tend to limit services, offer fewer covered benefits, and have relatively small provider networks. These limitations can impair access to quality care.27 New York can take steps as part of coverage expansion proposals to improve access to the same health care products and services, regardless of coverage source. For example, one proposed California plan, AB 8, provides for the Insurance Commissioner to approve no more than five standardized plans for both public and private insurance markets, allowing patients to make fully-educated decisions about both the cost and quality of benefits each plan will provide.28
Improving and streamlining enrollment procedures for public health insurance programs
Racial and ethnic minorities and immigrants are underrepresented, relative to eligibility rates, in public health insurance programs. States that have achieved greater success in increasing minority participation in public programs have developed and sustained aggressive outreach programs and have taken steps to improve and streamline enrollment, with particular attention to the needs of cultural and language-minority groups.29 New York can improve and streamline enrollment through policies that evaluate and improve enrollment procedures among eligible yet underserved groups. For example, New York can utilize media campaigns, community-based outreach and application assistance, identification of potential enrollees through other systems (such as school lunch, early childhood education, etc.), and simplified enrollment systems.
Consistently evaluating outreach to and enrollment of underserved groups in public health insurance programs
Measurement of public insurance take-up rates in low-income communities and communities of color is an important step to ensure that health care expansion efforts reach underserved groups. By regularly conducting such evaluations and responding to gaps and shortfalls, New York can expect to see improved coverage rates among eligible populations.30
II. Quality of Care
New York seeks to expand health care quality, as well as access. The State can provide incentives for quality improvement, such as pay-for-performance programs, performance measurement, and report cards. But quality improvement efforts that fail to take into account the different challenges and needs of underserved communities, and the health care institutions that serve them, can unintentionally worsen health care quality gaps. To prevent unintentional exacerbation of inequities, New York should establish mechanisms for promoting equity and accountability by promoting the collection of data on health care access and quality by patients’ race, ethnicity, income or education level, and primary language, and by publicly reporting this information.
New York can establish mechanisms for ensuring quality care and accountability to all communities by:
Requiring public and private health systems to collect data revealing and monitoring racial/ethnic, language status, and income-based health care disparities
Currently, state data collection efforts with regard to health care disparities are uneven. New York requires recipients of state funding (e.g., Medicaid managed care organizations) to collect and report health care access and quality data by patient demographic factors, but fails to utilize its leverage as a regulator, payer, and plan purchaser to require all health systems to collect and report data using consistent standards.31 And given that New York has non-discrimination laws that apply to health care settings and require state diligence to enforce, requirements to collect and report standardized data are an important benchmark for efforts to reduce health care inequality. New York should ensure that state health care expansion proposals mandate participation by all health systems operating in the state in a standardized data collection program.
Publicly reporting health care access and quality disparities
Once New York has obtained health care access and quality data by patient demographic characteristics, this information should be publicly reported, to promote greater public accountability, to allow consumers to make more informed decisions about where to seek care, and to assist state efforts to appropriate action to investigate potential violations of law.32
Encouraging the adoption of quality improvement programs that consider the health care challenges and needs of underserved communities
State health care quality improvement efforts, such as pay-for-performance or performance measurement, are gaining increasing attention. But because underserved communities typically face greater health needs and barriers to treatment, performance measurement that is blind to the additional challenges in providing health care to these communities can inadvertently dampen provider enthusiasm for treating low-income communities or communities of color. Quality improvement efforts should take into account the challenges and needs of underserved communities and reward efforts that reduce disparities and improve patient outcomes relative to baseline measures.33 New York should ensure that health care expansion proposals emphasize disparities reduction efforts and avoid unfairly penalizing providers in underserved communities while holding them and health systems accountable for improvements in health outcomes.
III. Patient Empowerment
Patients should be empowered to make decisions about their health care and to insist that care be delivered in a manner consistent with their health care needs, economic status, and cultural context. These issues are particularly relevant for racial and ethnic minority and immigrant patients, who may face significant cultural barriers in U.S. health care settings.34 These concerns can be addressed by:
Developing and strengthening patient education programs that are well-researched and are tailored to the need of underserved communities
Patient education programs commonly seek to help patients understand how to best access health care services and participate fully in treatment plans. Such efforts to empower patients can help reduce health care disparities by providing patients with skills to effectively navigate health care systems and ensure that their needs and preferences are met. For example, patient education programs have been found to be effective as a means of reducing racial and ethnic disparities in pain control.35 Patient education programs are most effective when designed in partnership with community members and groups and when language, culture, and other concerns faced by communities of color are fully addressed.36
Supporting and expanding community health worker programs
Community health workers, also known as lay health navigators or promotoras, are trained members of medically underserved communities who work to improve community health outcomes. Community health worker programs train individuals to teach disease prevention, conduct simple assessments of health problems, and help their neighbors access appropriate health and human resources.37 New York State currently has 23 community health work programs, focused on prenatal and early childhood health.38 Research and practice indicate that such services can improve patients’ ability to access care and understand how to manage illness. Most importantly, community health workers can help reduce health disparities by community mistrust of health care providers stemming from historical discrimination, breaking down cultural divides between providers and patients, assisting in obtaining health insurance and accessing care, and disseminating vital health information to underserved communities.39 From a health care system perspective, community health workers also improve quality and reduce costs by encouraging more appropriate use of health care resources and reducing uncompensated care.40 New York can build on the successes of its existing perinatal community health worker programs by providing grants, seed funding, or other resources to help stimulate community health worker programs in new areas of health disparities, such as diabetes, HIV/AIDS, and preventable ambulatory care sensitive conditions such as asthma, hypertension, and pneumonia.
IV. State Health Care Infrastructure
The disproportionate lack of health insurance among racial and ethnic minorities is associated with lower levels of health care resources (e.g., practitioners, hospitals and health care centers) in communities of color. Even if New York achieves universal health insurance coverage, communities of color will still require investments to improve their health care infrastructure.
New York can ensure that the community-level health care infrastructure needs of racial, ethnic, and language minority patients are better addressed by:
Supporting “safety net” hospitals and community health centers, and reducing the financial vulnerability of health care institutions serving poor and minority communities
People of color, immigrants and low-income individuals are more likely than other populations to access health care in safety net institutions, such as public hospitals and community health centers.41 In many cases, these institutions face financial vulnerability because of low Medicaid reimbursement rates and/or the costs of providing uncompensated care to uninsured individuals.42 These institutions may fare better in states where near-universal health insurance coverage proposals are enacted and where health insurance expansions are realized, but they will likely continue to face financial vulnerability until universal and equitable coverage is achieved.
New York operates a free care/bad debt pool aimed at reimbursing hospitals for uncompensated care. Yet the U.S. Department of Health and Human Services has said that many of New York’s most financially troubled hospitals will go bankrupt or default on their loans without more state assistance.43 State health care expansion proposals should include provisions to provide additional financial resources or other support to safety net institutions, particularly until coverage plans “ramp up” to reach uninsured populations. The viability of these institutions is particularly important if New York fails to establish truly “universal” coverage due to exclusion of childless adults or undocumented immigrants who are not eligible for Medicaid and are subject to enrollment caps in many state-funded programs—exclusions which we recommend against. In such a scenario, New York would likely rely on safety net institutions to provide a significant uninsured population with primary and preventative health care that is essential to the state’s health.
Creating and/or improving incentives for health care professionals to practice in underserved communities
Low-income and minority communities often have the most pressing need for health care services, but they are served by a dwindling number of providers and institutions that lack resources to expand and improve services (Figure 2).44 New York can address this imbalance by providing incentives, such as funds for graduate medical education programs that focus on underserved populations, tuition reimbursement and loan forgiveness programs that require service in communities with health professional shortage areas.
V. State Program and Policy Infrastructure
New York can improve its capacity to plan for and address the health care policy challenges and needs of minority communities by adopting or strengthening existing policies such as:
Community health planning
Community health planning is a means of gaining community input and better aligning health care resources with community needs. Community health planning has a long history, but its promise as a tool to reduce health care disparities has yet to be fully realized. Community health planning seeks to strengthen communities to play a greater role in their own health, actively involving residents in the planning, evaluation, and implementation of health activities in their communities. The 1974 National Health Planning Law sought to create and support a network of community Health Systems Agencies (HSAs), but a lack of funding and effective mechanisms for community input to shape health policy has led to a decline of HSA power and influence.45
In New York, the laws creating a statewide Health Systems Agency remain on the books,46 though the State stopped funding the agency in the 1990s.47 Despite its decline, HSAs have been proven effective and significant tools for equity in New York. The Finger Lakes HAS (FLHSA), for example, has served as an important vehicle to address the common concerns of consumer groups, businesses, health plans, and providers regarding health planning.48 Through collaboration between the Rochester community, local businesses, and the local insurer, Blue Cross Blue Shield, FLHSA has remained an active, self-funded project, but requires greater funding support to remain a broad-based planning agency. New York can integrate strategies to restart and reinvigorate HSAs and include disparities reduction efforts as part of the mission of these planning agencies into its health care expansion proposals.
Certificate of Need assessment
Historically, the purpose of the Certificate of Need (CoN) process has been to control health care costs and ensure that capital and technology investments in the health care industry reflect community needs. In New York, the process has required hospitals and other health care institutions that seek to establish, expand or reduce services to submit proposals so that the Department of Health can evaluate projects to eliminate unnecessary duplication of services and ensure that investments strategically address health care needs. The CoN process, however, has great potential to encourage a better distribution of health care resources, reflecting community and statewide need.49 The four current criteria examined by the DOH through the CoN—public need, financial feasibility, character/competence and construction50—are necessary but insufficient to ensure reflection of community needs. Although DOH is required to assess public need in determining whether to grant a Certificate of Need application for the construction, expansion, or conversion of hospitals,51 the agency has not historically done so (Figure 3).52 New York should re-evaluate and reinvigorate the CoN process through new policies that ensure accountability for the use of public funds; reduce geographic, racial, ethnic and socioeconomic disparities; and reduce the “fragmentation” of the health insurance market. Specifically, New York should ensure that the collection of data revealing racial/ethnic, language status, and income-based health care disparities, discussed above, is integrated into the CoN process. DOH should make obtaining a Certificate of Need contingent on evidence that changes sought would reduce racial and economic health care inequality.53
Figure 3
Coordination between DOH, DOI, the New York State Division of Human Rights, and the Attorney General
The New York State Division of Human Rights is charged with reviewing complaints under the New York State Human Rights Law and enforcing the law. However, few complaints reviewed by the State Division address discrimination in access to health care.54 But because discrimination in health care is often covert, structural, and sometimes unintentional, review of these limited number of complaints are not alone a good way to discover and eliminate existing racial discrimination. The State Division should exercise its power to initiate its own investigations, file its own complaints, and conduct studies in compliance with state, federal and international human rights law and to prevent and eliminate discrimination in access to health care.55
To this end, New York should develop a comprehensive, statewide approach to eliminating racial and ethnic health disparities, grounded in the fundamental understanding that these disparities stem from historical, interpersonal and institutional racism. The State is empowered to eliminate health care gaps through its control of funding, power of regulation and control over the authorization of hospital closings and downsizing to control the allocation of health care resources. Moreover, the Attorney General possesses broad authority under parens patriae standing, which provides states with the ability to sue to protect the health of their residents.56 The Departments of Health and Insurance, the Office of the Attorney General, and the State Division of Human Rights should coordinate efforts to end health disparities based on race or ethnicity. One model of coordination is a bill pending before the Massachusetts legislature to establish an Office of Health Equity to coordinate all efforts to eliminate racial and ethnic discrimination in health care.57 An equally comprehensive government-led initiative in New York would need: (1) to share the honesty of the Massachusetts Commission to End Racial and
Ethnic Health Disparities58 in acknowledging that racial and ethnic health disparities are caused by racism and institutional tolerance of racial bias; (2) to be led by influential policymakers who could implement the recommendations into law; and (3) to examine and address the multiple causes of disparities, including health care services, patient education and behavior, and larger social conditions.59
VI. Policies to Address Social and Community-Level Determinants of Health
While largely outside of the purview of state health insurance coverage expansion proposals, any effort to reduce racial and ethnic health status gaps must address factors that lie largely outside of the health care arena. These include social and community-level determinants of health—such as environmental conditions in homes, employment, or educational institutions—which are powerful “upstream” predictors of who is healthy and who is ill. New York State health care reform proposals can consider strategies to:
Improve coordination of relevant state agencies that should address determinants (e.g., education, housing, employment)
State agencies that seek to reduce social and economic gaps are inherently engaging in health equity work. Almost all aspects of state policy in education, transportation, housing, commerce, and criminal justice influence the health of state residents, and can have a disproportionate impact on underserved communities. New York can take steps to coordinate the work of state agencies that impact health disparities, which would likely reduce duplication of effort, increase efficiency, and more effectively address health outcome disparities.
Health impact assessment (HIA) policies
HIA attempts to ensure that all government programs and initiatives in and outside of the health care delivery sector—such as transportation, housing, and environmental protection—are assessed to determine their potential impact on the health status of affected communities.60 HIA is used extensively as a policy and planning tool in Europe and other countries, and is used increasingly in the United States. The San Francisco Department of Public Health, for example, has developed and implemented the Healthy Development Measurement Tool to identify and assess community health needs and understand how land use and development projects can complement public health goals. New York should determine whether state health care expansion proposals include use of health impact assessments to assist planning.
Conclusion
New York is synonymous with opportunity in the American vocabulary. In considering health care system proposals, we ask that you evaluate not only whether a greater number of residents will be insured, but also whether system reform proposals improve the equal opportunity of New York residents to access quality health care. We hope the equity benchmarks laid out above will assist in your evaluation process.
Notes:
1. N.Y. CONST. art. XVII, §§ 1, 3.
2. Civil Rights Act of 1964, tit. VI, 42 U.S.C. §2000d et seq.; Civil Rights Act of 1964, tit. VII, 42 U.S.C. §2000e et seq.; Nondiscrimintion Under Programs Receiving Federal Assistance Through the Department of Health and Human Services Effectuation of Title VI of the Civil Rights Act of 1964, 45 C.F.R. §80.3 (2005); Guidance to Federal Financial Recipients Regarding Title VI Prohibition Against National Origin Discrimination Affecting Limited English Proficient Persons, 68 Fed. Reg. 47311 (2003)
2. International Convention on the Elimination of All Forms of Racial Discrimination, Dec. 21, 1965, 140 CONG. REC. 14326, 660 U.N.T.S. 195.
3. Medicaid Act, Pub. L. No. 89-97, tit. I, 79 Stat. 343 (1967); Hospital Survey and Construction Act (“Hill-Burton Act”), Pub. L. No. 88-443, 78 Stat. 447, 42 U.S.C. §§ 291-291(o) (1964).
4. Poll designed by Harvard School of Public Health and conducted by The Opportunity Agenda from October 24th to November 13th, 2006, with a representative sample of 479 New York State residents over the age of 18. The margin of error is +/-4.48% at the 95% confidence level.
5. N.Y. CONST. art. XVII, §3.
6. N.Y. CONST. art. XVII, §3. The text of the public health provision makes clear that it covers both the “protection” and the “promotion” of health, that it covers all “inhabitants” of the State, and that provision for such protection and promotion by state and municipal governments is mandatory. Courts have generally found that use of the term “shall” establishes a mandate. See, e.g., Nat’l Ass’n of Home Builders v. Defenders of Wildlife, 127 S. Ct. 2518, 2531-32 (2007) (finding the statutory language “shall approve” mandatory) (citing Lopez v. Davis, 531 U.S. 230, 241 (2001) (noting Congress'”use of a mandatory ‘shall’ . . . to impose discretionless obligations”); Lexecon Inc. v. Milberg Weiss Bershad Hynes & Lerach, 523 U.S. 26, 35 (1998) (“The mandatory ‘shall’ . . . normally creates an obligation impervious to judicial discretion”); Association of Civil Technicians v. FLRA, 22 F.3d 1150, 1153 (D.C. Cir. 1994) (“The word ‘shall’ generally indicates a command that admits of no discretion on the part of the person instructed to carry out the directive”); Black’s Law Dictionary 1375 (6th ed. 1990) (explaining that “[a]s used in statutes . . . this word is generally imperative or mandatory” and noting that in legal documents “shall” is construed as permissive only when necessary to carry out legislative intent or in cases where no right depends on its being taken in a mandatory sense). As the section of the state constitution on state finance explains: “Subject to the limitations on indebtedness and taxation, nothing in this constitution contained shall prevent the legislature from providing . . . for the protection by insurance or otherwise, against the hazards of unemployment, sickness and old age.” NY CONST. art. VII § 8.
7. STATE COVERAGE INITIATIVES & ACADEMY HEALTH, STATE OF THE STATES: BUILDING HOPE AND RAISING EXPECTATIONS (2007).
8. Supra note 4.
9. INST. OF MEDICINE, CROSSING THE QUALITY CHASM: A NEW HEALTH SYSTEM FOR THE 21ST CENTURY (2001).
10. INST. OF MEDICINE, UNEQUAL TREATMENT: CONFRONTING RACIAL AND ETHNIC DISPARITIES IN HEALTH CARE (2003).
11. THE OPPORTUNITY AGENDA, DANGEROUS AND UNLAWFUL: WHY OUR HEALTH CARE SYSTEM IS FAILING NEW YORK AND HOW TO FIX IT 42 (2006), available here.
12. Id. at 4.
13. Id.
14. U.S. CENSUS BUREAU, INCOME, POVERTY, AND HEALTH INSURANCE COVERAGE IN THE US: 2006 (2007).
15. D. HOLAHAN ET AL., UNITED HOSPITAL FUND, HEATH INSURANCE COVERAGE IN NEW YORK, 2001 (2003).
16. THE OPPORTUNITY AGENDA, DANGEROUS AND UNLAWFUL, supra note 11.
17. INST. OF MEDICINE, UNEQUAL TREATMENT, supra note 10.
18. Id..
19. See, e.g., M.M. Doty & A.L. Holmgren, Health care disconnect: gaps in coverage and care for minority adults. Findings from the Commonwealth Fund Biennial Health Insurance Survey, 2005 (Commonwealth Fund, Issue Brief, 2006); J.L. Hargraves & J. Hadley, The contribution of insurance coverage and community resources to reducing racial/ethnic disparities in access to care, 38 HEALTH SERVS. RESEARCH 809, 809-29 (2003); M. Lillie-Blanton & C. Hoffman, The role of health insurance coverage in reducing racial/ethnic disparities in health care, 24 HEALTH AFFAIRS 398, 398-408 (2005); R.M. Weinick et al., Who can’t pay for health care?, 20 J. OF GEN. INTERNAL MED. 504, 504-09 (2005).
20. MELVIN L. OLIVER & THOMAS M. SHAPIRO, BLACK WEALTH, WHITE WEALTH (1997).
21. Kathryn Pitkin Derose et al., Immigrants and Health Care: Sources of Vulnerability, 26 Health Affairs 1285, 1258-68 (2007).
22. C. Brach & I. Fraser, Reducing disparities through culturally competent health care: an analysis of the business case, 10(4) QUALITY MGMT. IN HEALTH CARE 15-28 (2002).
23. OFFICE OF MINORITY HEALTH, U.S. DEP’T OF HEALTH & HUMAN SERVS., NATIONAL STANDARDS FOR CULTURALLY AND LINGUISTICALLY APPROPRIATE SERVICES IN HEALTH CARE.
24. Id. at 10-13. All recipients of federal funds are mandated to meet Standards 4, 5, 6, and 7, which are based on Title VI of the Civil Rights Act as applied to Limited English Proficiency (LEP) persons. Standard 4 requires provision of bilingual staff and interpreter services at all hours to LEP persons. Standard 5 requires provision of oral offers and written notices to patients, in their preferred language, of their right to receive language assistance services. Standard 6 requires competence of language service providers and discourages the use of friends or family. Standard 7 requires materials and signage posted in the service area in languages of commonly encountered language populations.
25. INST. OF MEDICINE, IN THE NATION’S COMPELLING INTEREST: ENSURING DIVERSITY IN THE HEALTH CARE WORKFORCE (2004).
26. S.L Taylor & N. Lurie, The role of culturally competent communication in reducing ethnic and racial healthcare disparities, 10 AM. J. OF MANAGED CARE Spec. No.:SP1-4 (2004)
27. INST. OF MEDICINE, UNEQUAL TREATMENT (2003).
28. Cal. AB 8, 2007-08 Reg. Sess., § 1366.10 (2007).
29. C. Brach et al., Who’s enrolled in the State Children’s Health Insurance Program (SCHIP)? An overview of findings from the Child Health Insurance Research Initiative (CHIRI), 112 PEDIATRICS e499 (2003); D.C. Ross & I.T. Hill, Enrolling eligible children and keeping them enrolled, 13 FUTURE CHILD 81, 81-97 (2003); M.C. Morreale & A. English, Eligibility and enrollment of adolescents in Medicaid and SCHIP: recent progress, current challenges, 32 J. OF ADOLESCENT HEALTH 25, 25-39 (2003).
30. L.P. Shone et al., The role of race and ethnicity in the State Children’s Health Insurance Program (SCHIP) in four states: are there baseline disparities, and what do they mean for SCHIP?, 112 PEDIATRICS e521 (2003).
31. R.T. Perot & M. Youdelman, Racial, ethnic and primary language data collection in the health care system: An assessment of federal policies and practices (Commonwealth Fund, Commonwealth Fund Publication No. 492, Sept. 2001). S.D. Watson, Equity measures and systems reform as tools for reducing racial and ethnic disparities in health care (Commonwealth Fund, Commonwealth Fund Publication No. 776, Aug. 2005).
32. R.T. Perot & M. Youdelman, supra note 21; INST. OF MEDICINE, UNEQUAL TREATMENT (2003).
33. P.L. Casalino & A. Elster, Will Pay-For-Performance and quality reporting affect health care disparities?, 26 HEALTH AFFAIRS w405-14; R.G. Hood, Pay-For-Performance—Financial Health Disparities and the Impact on Healthcare Disparities, 99 J. OF THE NAT’L MED. ASS’N 953, 953-58 (2007).
34. INST. OF MEDICINE, UNEQUAL TREATMENT (2003).
35. D. Kalauokalani et al., Can patient coaching reduce racial/ethnic disparities in cancer pain control? Secondary analysis of a randomized controlled trial, 8 PAIN MED. 17, 17-24 (2007).
36. INST. OF MEDICINE, UNEQUAL TREATMENT (2003).
37. H.P. Freeman, Patient navigation: a community centered approach to reducing cancer mortality, 21 J. CANCER EDUC. Suppl. S11, S11-14 (2006); M.L. Steinberg et al., Lay patient navigator program implementation for equal access to cancer care and clinical trials: essential steps and initial challenges, 107 Cancer 2669, 2669-77 (2006). 38 N.Y. State Dep’t of Health, Community Health Worker Program.
39. COMMUNITY VOICES, COMMUNITY HEALTH WORKERS AND COMMUNITY VOICES: PROMOTING GOOD HEALTH (2003).
40. Id. at 13-14.
41. Kaiser Comm’n on Medicaid & the Uninsured, Stresses to the Safety Net: The Public Hospital Perspective, June 2005; J. Hadley et al., Would safety- net expansions offset reduced access resulting from lost insurance coverage? Race/Ethnicity differences, 25 HEALTH AFFAIRS 1679 (2006). Also note that New York provides Medicaid coverage to eligible documented immigrants, increasing the importance of safety-net institutions for many New Yorkers. Aliessa v. Novello, 96 N.Y.2d 418 (2001).
42. D.P. Andrulis, L.M. Duchon, SUNY Downstate Med. Ctr., Hospital care in the 100 largest cities and their suburbs, 1996-2002: Implications for the future of the hospital safety net in metropolitan America, Aug. 2005.
43. HHS was called the “Department of Housing and Urban Development” at the time of the statement. N.Y. State Assembly, Press Release, Health Care Reform Act of 2000 (1999).
44. P. Cunningham, Mounting pressures: physicians serving Medicaid patients and the uninsured, 1997-2001 (Center for Studying Health System Change, Tracking Report No. 6, Dec. 2002); P. Cunningham & J. May, Medicaid patients increasingly concentrated among physicians (Center for Study Health System Change, Tracking Report No. 16, Aug. 2006).
45. D.A. Conrad, Community care networks: linking vision to outcomes for community health improvement, 60 MED. CARE: RESEARCH & REV. Suppl. 95, 95-129 (2003); S. Sofaer, Community health planning in the United States: a postmortem, 10(4) FAMILY & COMMUNITY HEALTH 1, 1-12 (1988); R. Weech-Maldonado et al., Evaluating the effectiveness of community health partnerships: a stakeholder accountability approach, 26 J. OF HEALTH & HUMAN SERVS. ADMIN. 58, 58-92 (2003); L.B. LANDRUM, HEALTH PLANNING IS ALIVE AND WELL, AM. HEALTH PLANNING ASS’N.
46. N.Y. PUB. HEALTH § 2904-b.
47. Calling Upon the Legislature of the State of New York to Amend the Health Care Reform Act to Reauthorize Funding for Health Systems Agencies (Mar. 24, 1998); Judy Wessler, Comm’n on the Public’s Health System, Press Advisory, The Need for Health Planning (undated; on file with Judy Wessler, Comm’n on the Public’s Health System).
48. See Finger Lakes Health Systems Agency, Current Projects.
49. D.B. Smith, Eliminating Disparities in Treatment (Commonwealth Fund, Aug. 2005).
50. Public need considers the hospital’s impact on the specific population demographic regarding access to specific health services, facility utilization patterns and how the hospital will affect the epidemiology of certain relevant diseases in the community. Financial feasibility examines the hospital’s financial health, projected costs and potential profits/expenses regarding the specific project. Character/competence examines the hospital’s prior experience and success in operating a healthcare facility. Finally, construction deals with the hospital’s adherence to pertinent New York State regulations regarding the building of healthcare facilities.
51. In determining whether an application for construction, expansion, conversion should be granted, DOH is required to consider public need, as well as financial feasibility, character and competence, and construction. In determining whether to revoke an operating certificate, DOH is also required to consider public need; but in its approval of voluntary closures DOH has argued that it need not consider health needs. See N.Y. State Dep’t of Health, Certificate of Need Review Criteria.
52. In the mid-1980s, in response to a Title VI complaint filed by Legal Services of New York and New York Lawyers for the Public Interest, DOH entered negotiations with advocates and agreed to add a form to its Certificate of Need application that would address concerns about access to health care. Telephone interview with Judy Wessler, Director, Commission on the Public’s Health System (Nov. 16, 2006). The form, at the time identified as Schedule 18, required health care facilities to address access to facilities, including language access, in their applications and obligated DOH to weigh such issues in deciding whether to approve applications. Id. Schedule 18 no longer addresses health care access issues; it now applies to Residential Health Care Facilities. N.Y. State Dep’t of Health, Schedule 16 – CON Forms Specific to Residential Health Care Facilities. But this requirement was only enforced for a short time, while legal and community groups reviewed DOH procedures. The parts of the current Certificate of Need application that address issues of access and public need must once again be reviewed and enforced. A specific schedule is designated for each Article 28 facility. Schedule 16 applies to hospitals and Schedule 17 applies to Diagnostic and Treatment Center. N.Y. State Dep’t of Health, Schedule 16 – CON Forms Specific to Hospitals; N.Y. State Dep’t of Health, Schedule 16 – CON Forms Specific to Diagnostic and Treatment Centers (D&TC). Only Schedule 16 appears to require a facility access analysis for hospitals. See N.Y. State Dep’t of Health, Schedule 16 – CON Forms Specific to Hospitals, supra.
53. DAVID BARTON SMITH, ELIMINATING DISPARITIES IN TREATMENT AND THE STRUGGLE TO END SEGREGATION
(2005) (“Currently, specialized services such as open-heart surgery are moving from the inner suburbs of most urban areas to the outer ones, following white flight and urban sprawl. Market and convenience justifications mask a resegregation of care that increases the cost of health care and reduces its quality.”).
54. In Fiscal Year 2002-2003 only 2.8% of the complaints filed with the State Division complained of discrimination in public accommodations; in Fiscal Year 2003-2004, the number increased slightly to 3.1%. N.Y. State Div. of Human Rights, Annual Report, Website Ed., Fiscal Years 2002/2003-2003/2004.
55. The Division is empowered to develop human rights plans and policies for the state and to assist in their execution. The Division may convene “advisory councils, local, regional or state-wide . . . to study the problems of discrimination in all or specific fields of human relationships or . . . specific instances of discrimination because of age, race, creed, color, national origin, sexual orientation, military status, sex, disability[,] or marital status and [to] make recommendations to the division for the development of policies and procedures.” N.Y. EXEC. LAW § 295(8) (2006); see also N.Y. EXEC. LAW § 295(6)(b) (2006); N.Y. EXEC. LAW § 295(9) (2006); 18 N.Y. JUR. CIV. RTS. § 14 (2006).
56. DENNIS D. PARKER, STATE REFORM STRATEGIES, IN AWAKENING FROM THE DREAM 317, 322 (Denise Morgan, et al., eds., 2006). States have brought civil rights cases alleging discrimination in housing, public accommodations, access to health care, and employment, under parens patrie standing.
57. H. 2234, 185th Gen. Court (Ma. 2007).
58. A 3-year project that brought together legislators, community members, and experts in health and health care. Comm’n to End Racial & Ethnic Health Disparities, Final Report (Aug. 2007).
59. Id.
60. A.L. Dannenberg et al., Growing the field of health impact assessment in the United States: an agenda for research and practice, 96 Am. J. of Public Healt 262, 262-70 (2006).
This website uses cookies so that we can provide you with the best user experience possible. Cookie information is stored in your browser and performs functions such as recognising you when you return to our website and helping our team to understand which sections of the website you find most interesting and useful.
Strictly Necessary Cookies
Strictly Necessary Cookie should be enabled at all times so that we can save your preferences for cookie settings.
If you disable this cookie, we will not be able to save your preferences. This means that every time you visit this website you will need to enable or disable cookies again.